
COVID-19 Tx Guideline Test: Remdesivir with Forest Plots
Published by IDSA
Update History
May 3, 2021
Version 4.2.1 has been released and contains endorsement from the Pediatric Infectious Diseases Society.
April 14, 2021
April 5, 2021
March 18, 2021
Version 4.1.1 has been released and contains a revision to the number of studies found for ivermectin.
March 5, 2021
Version 4.1.0 has been released and contains a new recommendation on the use of bamlanivimab with etesevimab among ambulatory patients.
February 22, 2021
Version 4.0.0 has been released and contains a revised recommendation on the use of tocilizumab.
February 18, 2021
Version 3.10.0 has been released and includes additional information on study eligibility for ivermectin.
February 10, 2021
Version 3.9.0 has been released and contains an updated literature review for tocilizumab.
February 5, 2021
Version 3.8.0 has been released and includes two new recommendations on the use of ivermectin.
February 3, 2021
Version 3.7.0 has been released and includes two new recommendations on the use of neutralizing monoclonal antibodies.
January 8, 2021
Version 3.6.0 has been realeased and includes new recommendations on the use of baricitinib and an updated literature review on hydroxychloroquine.
December 2, 2020
Version 3.5.1 has been released and includes endorsement from the Pediatric Infectious Diseases Society.
November 22, 2020
Version 3.5.0 has been released and includes revisions to the sections on lopinavir/ritonavir, tocilizumab, and remdesivir.
November 18, 2020
Version 3.4.0 has been released and contains a new recommendation on the use of bamlanivimab.
September 25, 2020
Version 3.3.0 has been released and contains revised and new recommendations for the use of dexamethasone and a revised recommendation against the routine use of tocilizumab.
September 21, 2020
Version 3.2.1 has been released and includes endorsement from the Pediatric Infectious Diseases Society.
September 15, 2020
Version 3.2.0 has been released and contains a new recommendation on the use of remdesivir in patients with more moderate disease.
September 4, 2020
Version 3.1.0 has been released and contains additional information on convalescent plasma as well new and updated narrative summaries of treatments undergoing evaluation.
August 28, 2020
Version 3.0.1 has been released and includes endorsement from the Pediatric Infectious Diseases Society.
August 20, 2020
Version 3.0.0 of the guideline has been released and contains revised recommendations on hydroxychloroquine and hydroxychloroquine plus azithromycin.
June 25, 2020
Version 2.1.0 of the guideline has been released and includes revised recommendations on corticosteroids.
June 22, 2020
Version 2.0.0 of the guideline has been released and contains:
- Revised recommendations on hydroxychloroquine and hydroxychloroquine plus azithromycin
- Revised recommendations for convalescent plasma for treatment of COVID-19
- New recommendations on the use of remdesivir
- New recommendations for famotidine (not addressed in the prior version)
April 21, 2020
Version 1.0.4 of the guideline has been released.
Overview of COVID-19 Treatment Guidelines (Summary Table)

NA: not applicable/not reviewed; MV: mechanical ventilation; ECMO: extracorporeal membrane oxygenation; R: remark; AE: adverse events
*Chloroquine is considered to be class equivalent to hydroxychloroquine.
**Dexamethasone 6 mg IV or PO for 10 days (or until discharge) or equivalent glucocorticoid dose may be substituted if dexamethasone unavailable. Equivalent total daily doses of alternative glucocorticoids to dexamethasone 6 mg daily are methylprednisolone 32 mg and prednisone 40 mg.
***Patients at increased risk, see EUA at https://www.fda.gov/media/143603/download
****For hospitalized patients who cannot receive corticosteroids because of a contraindication
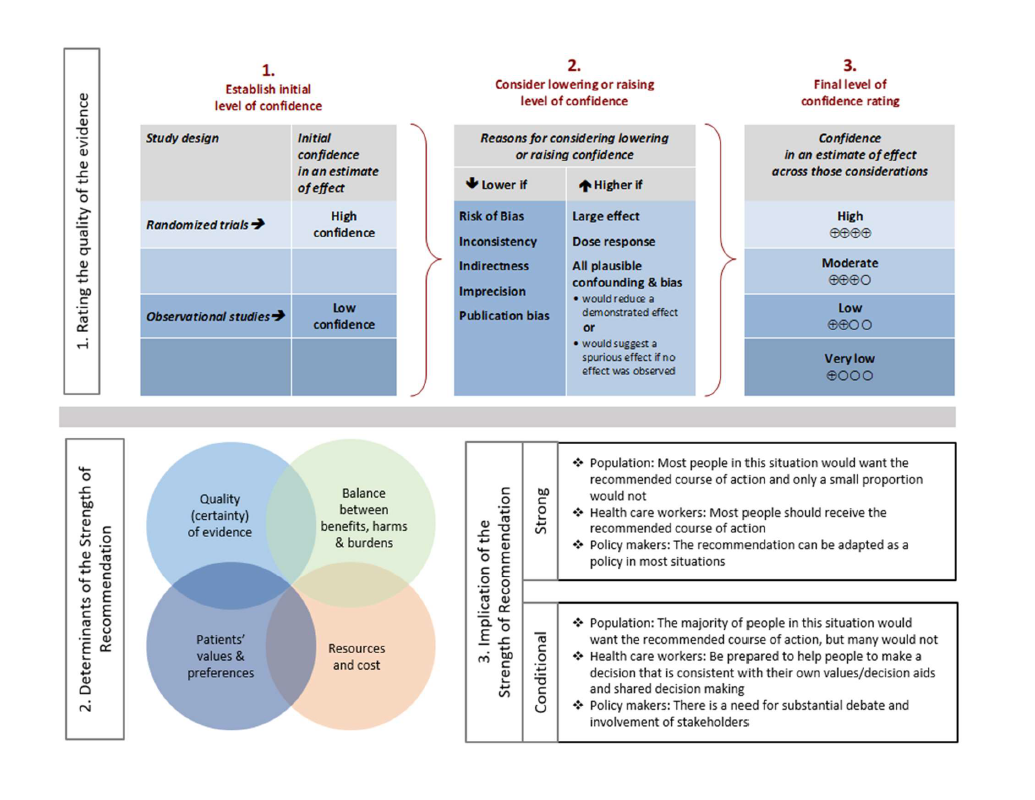
Strengths of recommendation
Recommend (strong recommendation): Guideline panel is confident that the desirable effects of an intervention outweigh the undesirable effects. Most or all individuals will be best served by the recommended course of action.
Suggest (weak or conditional recommendation): Guideline panel after discussion concludes that the desirable effects probably outweigh undesirable effects, but appreciable uncertainty exists. Not all individuals will be best served by the recommended course of action and the caregiver needs to consider more carefully than usual the individual patient’s circumstances, preferences, and values.
Certainty of evidence
⨁⨁⨁⨁ high
⨁⨁⨁◯ moderate
⨁⨁◯◯ low
⨁◯◯◯ very low
See Figure 1 in the Executive Summary.
Abstract
Background: There are many pharmacologic therapies that are being used or considered for treatment of coronavirus disease 2019 (COVID-19). There is a need for frequently updated practice guidelines on their use, based on critical evaluation of rapidly emerging literature.
Objective: There are many pharmacologic therapies that are being used or considered for treatment of coronavirus disease 2019 (COVID-19). There is a need for frequently updated practice guidelines on their use, based on critical evaluation of rapidly emerging literature.
Methods: In March 2020, the Infectious Diseases Society of America (IDSA) formed a multidisciplinary guideline panel of infectious disease clinicians, pharmacists, and methodologists with varied areas of expertise. The process followed a rapid recommendation checklist. The panel prioritized questions and outcomes. Then a systematic review of the peer-reviewed and grey literature was conducted. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence and make recommendations.
Results: On April 11, 2020, IDSA released online initial treatment recommendations and narrative summaries of other treatments under evaluation. Since that time, the guideline panel and methodologists have continued to monitor the literature and issue updates and addendums to these guidelines in response to evolving research.
Conclusions: Since the inception of its work, the panel has expressed the overarching goal that patients be recruited into ongoing trials, which would provide much needed evidence on the efficacy and safety of various therapies for COVID-19, given that we could not make a determination whether the benefits outweigh harms for most treatments.
Keywords: coronavirus, SARS-CoV-2, COVID, COVID-19, pneumonia
Executive Summary and Background
Executive Summary
Coronavirus disease 2019 (COVID-19) is a pandemic with a rapidly increasing incidence of infections and deaths. Many pharmacologic therapies are being used or considered for treatment. Given the rapidity of emerging literature, the Infectious Diseases Society of America (IDSA) identified the need to develop living, frequently updated evidence-based guidelines to support patients, clinicians and other health-care professionals in their decisions about treatment and management of patients with COVID-19.
Summarized below are the recommendations with comments related to the clinical practice guideline for the treatment and management of COVID-19. A detailed description of background, methods, evidence summary and rationale that support each recommendation, and research needs can be found online in the full text. In brief, per Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology, recommendations are labeled as “strong” or “conditional”. The word “recommend” indicates strong recommendations and “suggest” indicates conditional recommendations. In situations where promising interventions were judged to have insufficient evidence of benefit to support their use and with potential appreciable harms or costs, the expert panel recommended their use in the context of a clinical trial. These recommendations acknowledge the current “knowledge gap” and aim at avoiding premature favorable recommendations for potentially ineffective or harmful interventions.
- Recommendation 1: Among patients with COVID-19, the IDSA guideline panel recommends against hydroxychloroquine. (Strong recommendation, Moderate certainty of evidence)
- Remark: Chloroquine is considered to be class equivalent to hydroxychloroquine.
- Recommendation 2: Among hospitalized patients with COVID-19, the IDSA guideline panel recommends against hydroxychloroquine plus azithromycin. (Strong recommendation, Low certainty of evidence)
- Remark: Chloroquine is considered to be class equivalent to hydroxychloroquine
- Recommendation 3: Among hospitalized patients with COVID-19, the IDSA guideline panel recommends against the use of the combination lopinavir/ritonavir. (Strong recommendation, Moderate certainty of evidence)
- Recommendation 4: Among hospitalized critically ill patients* with COVID-19, the IDSA guideline panel recommends dexamethasone rather than no dexamethasone. (Strong recommendation, Moderate certainty of evidence)
- Remark: If dexamethasone is unavailable, equivalent total daily doses of alternative glucocorticoids may be used. Dexamethasone 6mg IV or PO for 10 days (or until discharge) or equivalent glucocorticoid dose may be substituted if dexamethasone unavailable. Equivalent total daily doses of alternative glucocorticoids to dexamethasone 6 mg daily are methylprednisolone 32 mg and prednisone 40 mg.
- *Critical illness is defined as patients on mechanical ventilation and ECMO. Critical illness includes end organ dysfunction as is seen in sepsis/septic shock. In COVID-19, the most commonly reported form of end organ dysfunction is ARDS
- Recommendation 5: Among hospitalized patients with severe**, but non-critical, COVID-19, the IDSA guideline panel suggests dexamethasone rather than no dexamethasone. (Conditional recommendation, Moderate certainty of evidence)
- Remark: Dexamethasone 6 mg IV or PO for 10 days (or until discharge) or equivalent glucocorticoid dose may be substituted if dexamethasone unavailable. Equivalent total daily doses of alternative glucocorticoids to dexamethasone 6 mg daily are methylprednisolone 32 mg and prednisone 40 mg.
- **Severe illness is defined as patients with SpO2 ≤94% on room air, including patients on supplemental oxygen.
- Recommendation 6: Among hospitalized patients with non-severe*** COVID-19 without hypoxemia requiring supplemental oxygen, the IDSA guideline panel suggests against the use of glucocorticoids. (Conditional recommendation, Low certainty of evidence)
- ***Non-severe illness is defined as patient with a SpO2 > 94% not requiring supplemental oxygen.
-
Recommendation 7: Among hospitalized adults with progressive severe* or critical** COVID-19 who have elevated markers of systemic inflammation, the IDSA guideline panel suggests tocilizumab in addition to standard of care (i.e., steroids) rather than standard of care alone. (Conditional recommendation, Low certainty of evidence)
- Remarks:
- Patients, particularly those who respond to steroids alone, who put a high value on avoiding possible adverse events of tocilizumab and a low value on the uncertain mortality reduction, would reasonably decline tocilizumab.
- In the largest trial on the treatment of tocilizumab, criterion for systemic inflammation was defined as CRP ≥75 mg/L.
- Remarks:
Severity definitions:
- *Severe illness is defined as patients with SpO2 ≤94% on room air, including patients on supplemental oxygen.
- **Critical illness is defined as patients on mechanical ventilation and ECMO. Critical illness includes end organ dysfunction as is seen in sepsis/septic shock. In COVID-19, the most commonly reported form of end organ dysfunction is ARDS.
-
Recommendation 8: Among patients hospitalized with COVID-19, the IDSA guideline panel suggests against COVID-19 convalescent plasma. (Conditional recommendation, Low certainty of evidence)
-
Recommendation 9: Among ambulatory patients with mild-to-moderate COVID-19, the IDSA guideline panel recommends COVID-19 convalescent plasma only in the context of a clinical trial. (Knowledge gap)
- Recommendation 10a: In hospitalized patients with severe* COVID-19, the IDSA panel suggests remdesivir over no antiviral treatment. (Conditional recommendation, Moderate certainty of evidence)
- *Severe illness is defined as patients with SpO2 ≤94% on room air
-
Recommendation 10b: In patients with COVID-19 on invasive ventilation and/or ECMO, the IDSA panel suggests against the routine initiation of remdesivir (Conditional recommendation, Very low certainty of evidence)
-
Recommendation 11: In patients on supplemental oxygen but not on mechanical ventilation or ECMO, the IDSA panel suggests treatment with five days of remdesivir rather than 10 days of remdesivir. (Conditional recommendation, Low certainty of evidence)
-
Recommendation 12: In patients with COVID-19 admitted to the hospital without the need for supplemental oxygen and oxygen saturation >94% on room air, the IDSA panel suggests against the routine use of remdesivir. (Conditional recommendation, Very low certainty of evidence)
-
Recommendation 13: Among hospitalized patients with severe COVID-19, the IDSA panel suggests against famotidine use for the sole purpose of treating COVID-19 outside of the context of a clinical trial. (Conditional recommendation, Very low certainty of evidence)
-
Recommendation 14: Among ambulatory patients with mild to moderate COVID-19 at high risk for progression to severe disease, the IDSA guideline panel suggests bamlanivimab/etesevimab or casirivimab/imdevimab rather than no neutralizing antibodies. (Conditional recommendation, low certainty of evidence)
- Remarks:
- Patients with mild to moderate COVID-19 who are at high risk of progression to severe disease admitted to the hospital for reasons other than COVID-19 may also receive bamlanivimab/etesevimab or casirivimab/imdevimab.
- Local variant susceptibility may be considered in the choice of the most appropriate neutralizing antibody therapy.
- There are limited data on efficacy of bamlanivimab/etesevimab or casirivimab/imdevimab in high-risk patients between 12 and 18 years of age.
- Remarks:
-
Recommendation 15: Among hospitalized patients with severe COVID-19, the IDSA guideline panel recommends against bamlanivimab monotherapy. (Strong recommendation, Moderate certainty of evidence)
-
Recommendation 16: Among hospitalized adults with severe* COVID-19 having elevated inflammatory markers but not on invasive mechanical ventilation, the IDSA panel suggests baricitinib rather than no baricitinib. (Conditional recommendation, Moderate certainty of evidence)
- Remarks:
- Baricitinib 4 mg per day up to 14 days or until discharge from hospital.
- Baricitinib appears to demonstrate the most benefit in those with severe COVID-19 on high-flow oxygen/non-invasive ventilation at baseline
-
Recommendation 17: Among hospitalized patients with severe* COVID-19 who cannot receive a corticosteroid (which is standard of care) because of a contraindication, the IDSA guideline panel suggests use of baricitinib with remdesivir rather than remdesivir alone. (Conditional recommendation, Low certainty of evidence)
- Remark: Baricitinib 4 mg daily dose for 14 days or until hospital discharge. The benefits of baricitinib plus remdesivir for persons on mechanical ventilation are uncertain.
-
Recommendation 18: In hospitalized patients with severe COVID-19, the IDSA panel suggests against ivermectin use outside of the context of a clinical trial. (Conditional recommendation, very low certainty of evidence)
-
Recommendation 19: In outpatients with COVID-19, the IDSA panel suggests against ivermectin use outside of the context of a clinical trial. (Conditional recommendation, very low certainty of evidence)
Since the inception of its work, the panel has expressed the overarching goal that patients be recruited into ongoing trials, which would provide much needed evidence on the efficacy and safety of various therapies for COVID-19. The panel has determined that when an explicit trade-off between highly uncertain benefits and known putative harms of these therapeutic agents were considered, a net positive benefit was not reached and could possibly be negative (risk of excess harm). The panel acknowledges that enrolling patients in randomized controlled trials (RCTs) might not be feasible for many frontline providers due to limited access and infrastructure. Should lack of access to clinical trials exist, we encourage setting up local or collaborative registries to systematically evaluate the efficacy and safety of drugs to contribute to the knowledge base. Each clinician can play a role in advancing our understanding of this disease through a local registry or other data collection efforts.
Background
The first cases of COVID-19 were reported from Wuhan, China in early December 2019 [1], now known to be caused by a novel beta-coronavirus, named as Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Within a span of months, COVID-19 has become pandemic due to its transmissibility, spreading across continents with the number of cases and deaths rising daily [2]. Although most infected individuals exhibit a mild illness (80%+), 14% have serious and 5% have critical illness. Approximately 10% will require hospital admission due to COVID-19 pneumonia, of which approximately 10% will require ICU care, including invasive ventilation due to acute respiratory distress syndrome (ARDS) [3]. While mortality appears to be more common in older individuals and those with comorbidities, such as chronic lung disease, cardiovascular disease, hypertension and diabetes, young people with no comorbidities also appear to be at risk for critical illness including multi-organ failure and death.
There has been an expanding number of studies rapidly published online and in academic journals; however, some of these may be of limited quality and are pre-published without sufficient peer-review. Critical appraisal of the existing studies is needed to determine if the existing evidence is sufficient to support currently proposed management strategies.
Given the rapid global spread of SARS-CoV-2 and the difficulty for the overburdened front-line providers and policymakers to stay up to date on emerging literature, IDSA has recognized the necessity of developing a rapid guideline for the treatment of COVID-19. The guideline panel is using a methodologically rigorous process for evaluating the best available evidence and providing treatment recommendations. Two additional guidelines on diagnostic testing and infection prevention also have been developed. These guidelines will be frequently updated as substantive literature becomes available and are accessible on an easy to navigate web and device interface at http://www.idsociety.org/covid19guidelines.
There continue to be several ongoing trials evaluating therapeutic agents for the treatment of COVID-19. As data becomes available from these trials and if there is a preponderance of evidence to suggest the use of a therapeutic agent even in the context of clinical trials is no longer warranted it will be removed from future updates of the guideline (and the removal will be noted in the updated guidelines). If there is emerging evidence on the efficacy or safety of a therapeutic agent not mentioned in the current version of the guideline it will be included in future updates of the guideline.
These recommendations are intended to inform patients, clinicians, and other health professionals by providing the latest available evidence.
Methods and Search Results
This guideline was developed using the GRADE approach for evidence assessment. In addition, given the need for an urgent response to a major public health crisis, the methodological approach was modified according to the Guidelines International Network/McMaster checklist for the development of rapid recommendations [4].
Panel Composition
The initial guideline panel assembled in March 2020 was composed of nine members including infectious diseases specialists as well as experts in public health as well as other front-line clinicians, specializing in pharmacology, pediatrics, medical microbiology, preventive care, critical care, hepatology, nephrology and gastroenterology. Organizational representatives were included from the Society for Healthcare Epidemiology of America (SHEA), and the Pediatric Infectious Diseases Society (PIDS). In May 2020, an additional panel member was included as a representative from the Society of Infectious Diseases Pharmacists (SIDP). The Evidence Foundation provided technical support and guideline methodologists for the development of this guideline.
Disclosure and Management of Potential Conflicts of Interest
The conflict of interest (COI) review group for this guideline includes two representatives from IDSA who are responsible for reviewing, evaluating and approving all disclosures. All members of the expert panel have complied with the COI process for reviewing and managing conflicts of interest, which requires disclosure of any financial, intellectual, or other interest that might be construed as constituting an actual, potential, or apparent conflict, regardless of relevancy to the guideline topic. The assessment of disclosed relationships for possible COI is based on the relative weight of the financial relationship (i.e., monetary amount) and the relevance of the relationship (i.e., the degree to which an association might reasonably be interpreted by an independent observer as related to the topic or recommendation of consideration). The COI review group has ensured that the majority of the panel and chair is without potential relevant (related to the topic) conflicts for the duration of their term on the panel. The chair and all members of the technical team have been determined to be unconflicted.
Question Generation
Clinical questions included in this guideline were developed into a PICO format (Population, Intervention, Comparison, Outcomes) [5] and prioritized according to available evidence that met the minimum acceptable criteria (i.e., the body of evidence reported on at least a case-series design, case reports were excluded). Panel members prioritized patient-important outcomes such as mortality, development of ARDS (need for non-invasive or invasive ventilation) and clinical improvement (such as disease-oriented outcomes inferred by radiological findings or virologic cure), and severe adverse events (SAE) leading to treatment discontinuation. Serious adverse events are death, life threatening reactions, those that require hospitalization, result in disability or permanent damage or require an intervention to prevent permanent impairment [6]. Additional drug specific harms were evaluated when clinically relevant, including possible drug-drug reactions, if applicable.
Search Strategy
The National Institute for Health and Care Excellence (NICE) highly-sensitive search was reviewed by the methodologist in consultation with the technical team information specialist and was determined to have high sensitivity [7]. An additional term, COVID, was added to the search strategy used in addition to the treatment terms identified in the PICO questions (Table s1). Ovid Medline and Embase were searched from 2019 through September 18, 2020. Horizon scans have been performed regularly during the evidence assessment and recommendation process to locate additional grey literature and manuscript pre-prints. Reference lists and literature suggested by panelists were reviewed for inclusion. No restrictions were placed on language or study type.
Screening and Study Selection
Two reviewers independently screened titles and abstracts, as well as eligible full-text studies. When acceptable RCTs of effectiveness were found, no additional non-randomized studies or non-comparative evidence (i.e., single arm case series) were sought. Evidence from single arm studies reporting on non-comparative rates of outcomes of interest were included if a historical control event rate could be estimated from the literature. Reviewers extracted relevant information into a standardized data extraction form.
For several interventions, no direct evidence was available other than case reports or mechanistic considerations. The panel either decided to include plausible indirect evidence and make a recommendation (e.g., from studies of SARS-CoV) or to provide a short narrative discussion of the intervention.
Data Collection and Analysis
Data extracted from the available evidence included: mortality, clinical progression or improvement as reported in the studies, virologic clearance, and adverse events. Where applicable, data were pooled using random effects model (fixed effects model for two or fewer trials or pooling of rates) using RevMan [8].
Risk of Bias and Certainty of Evidence
Risk of bias was assessed using the Cochrane Risk of Bias Tool for RCTs and the Risk of Bias Instrument for Non-randomized Studies – of Interventions (ROBINS-I) [9, 10]. The certainty of evidence was assessed using the GRADE approach [11]. Within GRADE, the body of evidence across each outcome is assessed for domains that may reduce or increase one’s certainty in the evidence. Factors that may reduce one’s certainty include risk of bias (study limitations), inconsistency (unexplained heterogeneity across study findings), indirectness (applicability or generalizability to the research question), imprecision (the confidence in the estimate of an effect to support a particular decision) or publication bias (selective publication of studies). One’s certainty in the evidence may be strengthened if the following considerations are present: large or very large magnitude of effect, evidence of a dose-response gradient, or opposing residual confounding. GRADE summary of findings tables were developed in GRADEpro Guideline Development Tool [12].
As higher quality direct evidence for clinical outcomes becomes available, outcomes previously deemed critical by the panel became less important for decision-making. For example, at the time of the first guideline, clinical improvement outcomes (e.g., need for mechanical ventilation) were not reported, only the results of radiographic findings. However, with the recent publication of RCTs and non-randomized studies reporting on direct measures of clinical improvement, results of radiographic studies were deemed to be less critical for decision making.
Evidence to Recommendations
The panel considered core elements of the GRADE evidence in the decision process, including Certainty of evidence and balance between desirable and undesirable effects. Additional domains were acknowledged where applicable (feasibility, resource use, acceptability). For all recommendations, the expert panelists reached consensus. Voting rules were agreed on prior to the panel meetings for situations when consensus could not be reached.
As per GRADE methodology, recommendations are labeled as “strong” or “conditional”. The words “we recommend” indicate strong recommendations and “we suggest” indicate conditional recommendations. Figure 1 provides the suggested interpretation of strong and weak recommendations for patients, clinicians, and healthcare policymakers. For recommendations where the comparators are not formally stated, the comparison of interest is implicitly referred to as “not using the intervention”. These recommendations acknowledge the current “knowledge gap” and aim at avoiding premature favorable recommendations for their use and to avoid encouraging the rapid diffusion of potentially ineffective or harmful interventions. Detailed suggestions about the specific research questions that should be addressed are found in the table (see Table s2).
Review Process
This guideline has been rapidly reviewed and approved by the IDSA Board of Directors Executive Committee external to the guideline development panel. SHEA and PIDS have reviewed and provided endorsement of its contents.
Updating Process
Regular, frequent screening of the literature will take place to determine the need for revisions based on the likelihood that any new data will have an impact on the recommendations. When necessary, the entire expert panel is reconvened to discuss potential changes.
Changes to these guidelines will fall into one of two categories: update or amendment. An update involves a search for new studies, and if any new studies are found, they will be critically appraisal and the pertinent section will be removed and replaced with the updated section. An amendment involves a change or correction to the document, without any search for new studies and their appraisal. It will also involve changes made to clarify or explain a section based on “living” feedback from the readers.
Guideline revisions may result in major, minor, or “patch” version changes, defined as follows:
- Major version (e.g., 1.0.0): Synonymous with a newly published version in the journal. This is usually called a "breaking version", i.e. prior recommendations may not be valid anymore.
- Minor version (e.g., 1.1.0): Includes new information, maybe even added PICOs, but not a breaking version, i.e., existing recommendations are still valid, although new recommendations may be available.
- Patch version (e.g., 1.0.1): Small changes, i.e., typos, adding words, removing words, but there are no material changes to the document or changes in recommendations.
Results
Systematic review and horizon scan of the literature identified 2030 references of which 48 informed the evidence base for these recommendations (Figure s1). Characteristics of the included studies can be found in the supplementary materials.
Recommendations 1 and 2: Hydroxychloroquine and Hydroxychloroquine + azithromycin
Section last reviewed and updated 12/23/2020
Last literature search conducted 12/14/2020
Recommendation 1. Among hospitalized patients with COVID-19, the IDSA guideline panel recommends against hydroxychloroquine*. (Strong recommendation, Moderate certainty of evidence)
- Remark: Chloroquine is considered to be class equivalent to hydroxychloroquine.
Recommendation 2. Among hospitalized patients with COVID-19, the IDSA guideline panel recommends against hydroxychloroquine* plus azithromycin. (Strong recommendation, Low certainty of evidence)
- Remark: Chloroquine is considered to be class equivalent to hydroxychloroquine.
Why are hydroxychloroquine and hydroxychloroquine plus azithromycin considered for treatment?
Hydroxychloroquine (HCQ) and chloroquine are 4-aminoquinoline drugs developed in the mid-20th century for the treatment of malaria [13]. Hydroxychloroquine differs from chloroquine only in the addition of a hydroxyl group and is associated with a lower incidence of adverse effects with chronic use [13]. Both drugs have been used in the treatment of autoimmune diseases because of their immunomodulatory effects on several cytokines, including interleukin-1 (IL-1) and IL-6 [13]. There is some evidence that these drugs also have antiviral properties against many different viruses, including the coronaviruses [14, 15]. They have demonstrated in vitro activity against SARS-CoV-2, which range considerably between studies, but are generally within the range of predicted achievable tissue concentrations [14, 16-18]. The in vitro activity, the extensive use for other conditions, and widespread availability of generic versions of the drug made it an attractive option for treatment of COVID-19. Interest in combinations of HCQ with azithromycin (AZ) began when investigators in a small, uncontrolled study of hydroxychloroquine use for COVID-19 noticed a higher frequency of patients achieving virologic response in the six subjects who received AZ to prevent bacterial infection [19]. Azithromycin, widely utilized as an antibacterial agent, has also been shown to have in vitro antiviral activity against a variety of ribonucleic acid viruses [20-22]. While the exact mechanism of antiviral activity is unknown, possibilities include inhibiting endocytosis and limiting viral replication [23] and the induction of interferon [22, 24]. Macrolides have also been shown to have anti-inflammatory activity [25, 26].
Summary of the evidence
Our search identified eight RCTs and seven comparative cohort studies of hospitalized patients with confirmed COVID-19 treated with HCQ with reported mortality, clinical progression or clinical improvement, and adverse events outcomes [27-41] (Table s3a) (Table 1).
In addition, we identified two RCTs, four comparative cohort studies, one case-control study, and three single-arm studies reporting adjusted analyses of hospitalized patients with confirmed COVID-19 treated with HCQ plus AZ with reported mortality, failure of virologic clearance (assessed with polymerase chain reaction [PCR] test), clinical improvement, and adverse events (i.e., significant QT prolongation leading to treatment discontinuation) [19, 27, 28, 37, 39, 41-45] (Table s3b) (Table 2).
Benefits
Hydroxychloroquine
Five RCTs showed a trend toward mortality among patients with COVID-19 treated with HCQ compared to those who were not (relative risk [RR]: 1.08; 95% confidence interval [CI]: 0.99, 1.19, Moderate certainty in the evidence) (Table 1) [28, 29, 33].
Hydroxychloroquine + Azithromycin
One RCT could not exclude the risk of in-hospital mortality among patients treated with HCQ+AZ compared to those not receiving HCQ or HCQ+AZ (hazard ratio [HR]: 0.64; 95% CI: 0.18, 2.21; Low certainty of evidence [CoE]) [28]. Three non-randomized studies failed to identify an association between treatment with HCQ+AZ and mortality: Ip reported an adjusted HR of 0.98 (95% CI: 0.75, 1.28); Magagnoli reported an adjusted HR in a subset after propensity score adjustment of 0.89 (95% CI: 0.45, 1.77); Rosenberg 2020 reported an adjusted HR of 1.35 (95% CI: 0.79, 2.40) [37, 39, 41]. As stated in the HCQ section, one non-randomized study reported a reduction in mortality among patients receiving HCQ+AZ (HR: 0.29; 95% CI: 0.22, 0.40); however, it failed to adjust for the critical confounder of disease severity and imbalances in steroid use [27]. As described in the HCQ section, similar methodologic concerns exist among patients allocated to HCQ+AZ in the Arshad study, leading to several sources of bias in interpreting their favorable results.
Harms
Hydroxychloroquine
One RCT reported that persons treated with HCQ experienced a longer time until hospital discharge (median 16 days compared with 13 days) and lower probability of being discharged alive within the 28-day study period (rate ratio: 0.92; 95% CI: 0.85, 0.99) [29]. In addition, persons treated with HCQ who were not on mechanical ventilation at baseline were more likely to be placed on mechanical ventilation during follow up (rate ratio: 1.10; 95% CI: 0.92, 1.31; Low CoE) [29, 32]. Across the body of evidence from four RCTs, treatment with HCQ may increase the risk of experiencing adverse events (RR: 2.36; 95% CI: 1.49, 3.75; Low CoE) and severe adverse events (adjusted odds ratio: 1.26; 95% CI: 0.56, 2.84; Low CoE) [28, 30, 31, 35]. One RCT and two non-randomized studies suggest increased risk of QT prolongation among patients treated with HCQ compared to those not receiving HCQ (RR: 8.47; 95% CI: 1.14, 63.03; Low CoE and RR: 2.89; 95% CI: 1.62, 5.16; Very low CoE, respectively) [28, 38, 39]. In addition, Rosenberg 2020 reported 16% of patients in the HCQ arm experienced arrhythmias compared with 10% in the non-HCQ arm (RR: 1.56; 95% CI: 0.97, 2.50; Very low CoE).
Gastrointestinal side effects occurred in 7% of patients in a prospective cohort study in 224 COVID-19 uninfected patients with systemic lupus erythematosus (SLE) who received either chloroquine or hydroxychloroquine for routine care [46].
While the 4-aminoquinolines, chloroquine and HCQ, have not been demonstrated to cause hemolysis in people with glucose-6-phosphate dehydrogenase (G6PD) deficiency [47, 48], case reports of hemolysis have emerged when these agents have been used for the treatment of COVID-19 [49-51]. It is possible that infection with SARS-CoV-2 may trigger hemolysis in G6PD deficient individuals in the absence of a 4-aminoquinolone. Caution should be exercised in administering these agents to G6PD deficient individuals with COVID-19, particularly if used for extended durations.
Renal clearance accounts for 15-25% of total clearance of HCQ; however, dose adjustments are not recommended with kidney dysfunction. Chloroquine and HCQ are metabolized by cytochrome P450 isoenzymes 2C8, 2D6, and 3A4 [52]. Therefore, inhibitors and inducers of these enzymes may result in altered pharmacokinetics of these agents.
Hydroxychloroquine + Azithromycin
One RCT suggests increased risk of QT prolongation among patients treated with HCQ+AZ compared to those not receiving HCQ (RR: 8.50; 95% CI: 1.16, 62.31; Low CoE) [28]. Two studies described significant QT prolongation in 10 of 95 patients treated with HCQ+AZ, illustrating the high risk for clinically relevant arrhythmias with this treatment [43, 45]. In addition, several case reports of QT prolongation related to HCQ have also been published [53-56]. A case-control study of persons with COVID-19 treated with HCQ+AZ compared to healthy, untreated controls reported higher values of minimum (415 vs. 376 ms), mean (453 vs. 407 ms) and maximum QTc-interval (533 vs. 452 ms) among COVID-19 cases (n=22) compared to controls (n=34) [42].
Additional case reports have cited the risk of a prolonged QT prolongation, torsades de pointes, and ventricular tachycardia in patients without COVID-19 receiving AZ alone. In a large cohort study, patients taking a five-day course of AZ had an increased risk of sudden cardiac death with a HR of 2.71 (1.58-4.64) vs. 0.85 (0.45-1.60), compared to patients receiving either no antibiotic or amoxicillin, respectively [57]. Given the cumulative effect on cardiac conduction seen with HCQ and AZ, if this combination was used, baseline and follow-up electrocardiogram (ECG) monitoring would be indicated, as well as careful surveillance for other concomitant medications known to prolong the QT interval.
Azithromycin has a low risk for cytochrome P450 interactions [58]; however, additional pharmacologic adverse events including gastrointestinal effects and QT prolongation need to be carefully considered, particularly in the outpatient setting where frequent ECG monitoring is not feasible.
Providers are encouraged to visit resources such as https://www.covid19-druginteractions.org/ to aid in the evaluation and management of drug interactions with current and emerging investigational agents for COVID-19.
Other considerations
The panel agreed that the overall certainty of evidence against treatment with HCQ was moderate due to concerns with imprecision around the risk for a trend towards harms from increased mortality. When considering the addition of AZ, the overall certainty of the evidence was low; however, the panel recognized even greater concern with the toxicity. In addition, based on the moderate certainty of increased QT prolongation, the panel determined that this demonstrated certain harm with uncertain benefit; therefore, the panel made a strong recommendation against HCQ+AZ.
Conclusions and research needs for this recommendation
The guideline panel recommends against the use of either HCQ alone or in combination with AZ in the hospital setting as higher certainty benefits (e.g., mortality reduction) are now highly unlikely even if additional high quality RCTs would become available.
This recommendation does not address the use of azithromycin for secondary bacterial pneumonia in patients with COVID-19 (Table s2).
Supplementary Information
Study Characteristics Tables:
- Table s3a. Hydroxychloroquine versus no hydroxychloroquine
- Table s3b. Hydroxychloroquine/azithromycin versus no hydroxychloroquine/azithromycin
Forest Plots:
- Figure s2a. Outcome of mortality point estimate demonstrates increased risk with hydroxychloroquine treatment
Figure s2b. Outcome of progression to mechanical ventilation demonstrates increased risk with HCQ treatment - Figure s2c. Outcome of adverse events demonstrates increased risk with hydroxychloroquine treatment
- Figure s2d. Outcome of QT prolongation demonstrates increased risk with hydroxychloroquine treatment
Risk of Bias Tables:
- Table s4a. RCTs (hydroxychloroquine ± azithromycin vs. no hydroxychloroquine ± azithromycin)
- Table s4b. Non-randomized studies (hydroxychloroquine ± azithromycin vs. no hydroxychloroquine ± azithromycin)
Recommendation 3: Lopinavir/ritonavir
Section last reviewed and updated 11/22/2020
Last literature search conducted 11/18/2020
Recommendation 3: Among hospitalized patients with COVID-19, the IDSA guideline panel recommends against the use of the combination lopinavir/ritonavir. (Strong recommendation, Moderate certainty of evidence)
The last literature search was conducted on November 18, 2020.
Why is lopinavir plus ritonavir considered for treatment?
Lopinavir/ritonavir is a protease inhibitor that was U.S. Food and Drug Administration (FDA)-approved for the treatment of HIV in September 2000. Ritonavir is added to the combination as a pharmacokinetic enhancer due to its strong inhibition of cytochrome P450 3A4, a metabolic pathway for lopinavir metabolism. Lopinavir/ritonavir demonstrated in vitro inhibition of SARS CoV-1 and MERS-CoV replication [59-61]. A trial of lopinavir/ritonavir and ribavirin vs historical controls in SARS CoV-1 patients, showed a reduced rate of ARDS and mortality in those receiving lopinavir/ritonavir. This study had limitations including a control group from early in the outbreak when management strategies likely differed significantly [62]. During the MERS outbreak, case reports cited efficacy of lopinavir/ritonavir with interferon in the management of MERS patients [63, 64]. During the early phase of COVID-19, triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin shortened the duration of viral shedding and hospital stay in patients with mild to moderate COVID-19 in an open-label, randomized, phase II trial [65].
Summary of the evidence
Three RCTs reported on treatment with combination lopinavir/ritonavir or placebo for hospitalized patients with COVID-19 [32, 66, 67] (Table 3). The trials reported on the following outcomes: mortality, failure of clinical improvement (measured using a 7-point scale or hospital discharge), need for mechanical ventilation, and adverse events leading to treatment discontinuation.
Benefits
Among hospitalized patients with COVID-19, treatment with lopinavir/ritonavir failed to show or exclude a beneficial effect on mortality or need for invasive mechanical ventilation (RR: 1.00; 95% CI: 0.89, 1.13; moderate certainty of evidence and RR: 1.12; 95% CI: 0.93, 1.34; low CoE). Similarly, lopinavir/ritonavir may reduce failure of clinical improvement at 14 days, but it is uncertain (RR: 0.78; 95% CI: 0.63, 0.97; very low CoE).
Harms
RECOVERY reported 1/1588 serious adverse event due to treatment with lopinavir-ritonavir [67]; however, nearly 14% of lopinavir/ritonavir recipients in Cao 2020 were unable to complete the full 14-day course of administration. This was due primarily to gastrointestinal adverse events, including anorexia, nausea, abdominal discomfort, or diarrhea, as well as two serious adverse events, both acute gastritis. Two recipients had self-limited skin eruptions. Such side effects, including the risks of hepatic injury, pancreatitis, more severe cutaneous eruptions, and QT prolongation, and the potential for multiple drug interactions due to CYP3A inhibition, are well documented with this drug combination. The side-effect profile observed in these trials raise concerns about the use of higher or more prolonged lopinavir–ritonavir dose regimens in efforts to improve outcomes.
Other considerations
The panel determined the certainty of evidence to be moderate due to concerns with imprecision. The guideline panel made a strong recommendation against treatment with the combination of lopinavir/ritonavir for hospitalized patients with COVID-19.
Conclusions and research needs for this recommendation
The guideline panel recommends against treatment with lopinavir/ritonavir in hospitalized patients with COVID-19.
Supplementary Information
Study Characteristics Table:
Forrest Plots:
- Figure s3a. Outcome of mortality at 28 days for lopinavir-ritonavir vs. no lopinavir-ritonavir
- Figure s3b. Outcome of invasive mechanical ventilation for lopinavir-ritonavir vs. no lopinavir-ritonavir
Risk of Bias Table:
Recommendations 4-6: Corticosteroids
Section last reviewed and updated 9/25/2020
Last literature search conducted 9/4/2020
Recommendation 4: Among hospitalized critically ill patients* with COVID-19, the IDSA guideline panel recommends dexamethasone rather than no dexamethasone. (Strong recommendation, Moderate certainty of evidence)
- Remark: If dexamethasone is unavailable, equivalent total daily doses of alternative glucocorticoids may be used. Dexamethasone 6 mg IV or PO for 10 days (or until discharge) or equivalent glucocorticoid dose may be substituted if dexamethasone unavailable. Equivalent total daily doses of alternative glucocorticoids to dexamethasone 6 mg daily are methylprednisolone 32 mg and prednisone 40 mg.
Recommendation 5: Among hospitalized patients with severe**, but non-critical, COVID-19 the IDSA guideline panel suggests dexamethasone rather than no dexamethasone. (Conditional recommendation, Moderate certainty of evidence)
- Remark: Dexamethasone 6 mg IV or PO for 10 days (or until discharge) or equivalent glucocorticoid dose may be substituted if dexamethasone unavailable. Equivalent total daily doses of alternative glucocorticoids to dexamethasone 6 mg daily are methylprednisolone 32 mg and prednisone 40 mg.
Recommendation 6: Among hospitalized patients with non-severe*** COVID-19 without hypoxemia requiring supplemental oxygen, the IDSA guideline panel suggests against the use of glucocorticoids. (Conditional recommendation, Low certainty of evidence)
Severity definitions:
- *Critical illness is defined as patients on mechanical ventilation and ECMO. Critical illness includes end organ dysfunction as is seen in sepsis/septic shock. In COVID-19, the most commonly reported form of end organ dysfunction is ARDS
- **Severe illness is defined as patients with SpO2 ≤94% on room air, including patients on supplemental oxygen.
- ***Non-severe illness is defined as patient with a SpO2 > 94% not requiring supplemental oxygen.
The last literature search was conducted on September 4, 2020 and we identified eight RCTs and seven comparative non-randomized studies.
Why are corticosteroids considered for treatment?
In the early days of the SARS-CoV-2 pandemic, based on experience in both SARS and MERS, recommendations [68] cautioned against the use of systemic corticosteroids due to risk of worsening clinical status, delayed viral clearance, and adverse events [69-71]. Given the hyper-inflammatory state in COVID-19, immunomodulatory approaches, including steroids, continue to be evaluated to address both ARDS and systemic inflammation. ARDS stemming from dysregulated systemic inflammation may translate into prolonged ventilatory requirements and in-hospital mortality. In non-viral ARDS settings there is increasing support for the role of steroids in the management of ARD [72]. A recent multicenter RCT in patients with moderate to severe ARDS demonstrated a reduced number of ventilatory days and reduction in mortality with use of a 10-day regimen of dexamethasone [73].
Summary of the evidence
Critical illness
Our search identified one systematic review that analyzed eight RCTs reporting on treatment with glucocorticoids among 1,844 critically ill patients with COVID-19 [74]. Three RCTs reported on patients treated with low- and high-dose dexamethasone [73, 75, 76]; three RCTs reported on patients treated with low-dose hydrocortisone [77-79]; and two RCTs reported on patients treated with high-dose methylprednisolone [74, 80]. The definition of critically ill varied across trials; however, the majority of patients had ARDS.
Severe and non-severe illness
Our search identified one RCT, one “partially” randomized trial, one prospective cohort, and five retrospective cohort studies [75, 81-87]. The RCT provided the best available evidence on treatment with corticosteroids for persons with COVID-19 [75] (Table 4, Table 5, and Table 6). Corral-Gudino et al. reported on a study that randomized patients to receive methylprednisolone or standard of care; however, patients expressing a preference for methylprednisolone were assigned to the same treatment arm [81]. Corral-Gudino et al. did not report the disaggregated results from the randomized trial; therefore, succumbing to the same potential for bias as reported subsequently for the non-randomized studies. The non-randomized studies had significant limitations with controlling for multiple co-interventions and disease severity at baseline [82-87]. All non-randomized studies had concerns with risk of bias due to lack of adjustment for critical confounders or potential for residual confounding. Timing of receipt, dose and duration of corticosteroids varied across studies.
The RECOVERY trial is a randomized trial among hospitalized patients in the United Kingdom [75]. In that study, 2,104 participants were randomized to receive dexamethasone (6 mg daily for up to 10 days) and 4,321 were randomized to usual care. The RECOVERY trial reported on the outcomes of mortality and hospital discharge. Participants and study staff were not blinded to the treatment arms.
Benefits
Critical illness
Among hospitalized, critically ill patients, the odds of mortality at 28 days was 34% less among patients treated with glucocorticoids than among patients not treated with glucocorticoids (OR: 0.66; 95% CI: 0.54; 0.82; High CoE). In addition, at 28 days, patients receiving dexamethasone were more likely to be discharged from the hospital (RR: 1.11; 95% CI: 1.04, 1.19; Moderate CoE).
Severe illness
Among hospitalized patients, 28-day mortality was 17% lower in the group that received dexamethasone than in the group that did not receive dexamethasone (RR 0.83; 0.74-0.92; Moderate CoE). In addition, at 28 days, patients receiving dexamethasone were more likely to be discharged from the hospital (RR: 1.11; 95% CI: 1.04, 1.19; Moderate CoE).
Non-severe illness
In a sub-group analyses of patients without hypoxia not receiving supplemental oxygen, there was no evidence for benefit and a trend toward harm with dexamethasone in participants who were not on supplemental oxygen (RR 1.22; 0.86, 1.75; Low CoE).
Harms
A systematic review of six studies did not report a difference in the events of serious adverse events experienced by patients randomized to receive treatment with glucocorticoids or no treatment with glucocorticoids (64/354 among those receiving glucocorticoids vs. 80/342 among those not receiving glucocorticoids).
Patients receiving a short course of steroids may experience hyperglycemia, neurological side effects (e.g., agitation/confusion), adrenal suppression, and risk of bacterial and fungal infection [82, 88, 89].
Other considerations
Critical illness
The panel agreed that the overall certainty of the evidence for treatment with glucocorticoids for patients with critical COVID-19 was moderate due to concerns with indirectness and imprecision.
Severe illness
The panel agreed the overall certainty of evidence for treatment with glucocorticoids for patients with severe COVID-19 as moderate due to concerns with indirectness since the evidence was from dexamethasone.
Non-severe illness
The panel agreed that the overall certainty of evidence for patients without hypoxemia requiring supplemental oxygen as low due to concerns with risk of bias (post hoc analysis) and imprecision.
The panel agreed the overall certainty of evidence for treatment with glucocorticoids for patients with severe COVID-19 as moderate due to concerns with indirectness since the evidence was from dexamethasone. The panel agreed that the overall certainty of evidence for patients without hypoxemia requiring supplemental oxygen as low due to concerns with risk of bias (post hoc analysis) and imprecision.
Conclusions and research needs for these recommendations
The guideline panel recommends dexamethasone for patients with critical COVID-19. The guideline panel suggests dexamethasone for patients with severe COVID-19. If dexamethasone is not available, then alternative glucocorticoids may be used (see details above). The guideline panel suggests against glucocorticoids for patients with COVID-19 without hypoxemia requiring supplemental oxygen.
Additional research is needed to inform the generalizability of treatment with different glucocorticoids for patients with COVID-19 (Table s2).
Supplementary Information
Study Characteristics Table:
Risk of Bias Table:
Recommendation 7: Tocilizumab
Section last reviewed and updated on 2/17/2021
Last literature search conducted 2/11/2021
Recommendation 7: Among hospitalized adults with progressive severe* or critical** COVID-19 who have elevated markers of systemic inflammation, the IDSA guideline panel suggests tocilizumab in addition to standard of care (i.e., steroids) rather than standard of care alone. (Conditional recommendation, Low certainty of evidence)
- Remarks:
- Patients, particularly those who respond to steroids alone, who put a high value on avoiding possible adverse events of tocilizumab and a low value on the uncertain mortality reduction, would reasonably decline tocilizumab.
- In the largest trial on the treatment of tocilizumab, criterion for systemic inflammation was defined as CRP ≥75 mg/L.
Severity definitions:
*Severe illness is defined as patients with SpO2 ≤94% on room air, including patients on supplemental oxygen.
**Critical illness is defined as patients on mechanical ventilation and ECMO. Critical illness includes end organ dysfunction as is seen in sepsis/septic shock. In COVID-19, the most commonly reported form of end organ dysfunction is ARDS.
Why is tocilizumab considered for treatment?
Some patients with COVID-19 develop a hyperinflammatory syndrome that is characterized by elevations in proinflammatory cytokines and multiorgan dysfunction also known as the immunopathology of SARS-CoV-2 infection. The significance of these findings is unclear, however early descriptions found that those with elevated IL-6 levels and evidence of hyperinflammation had increased rates of more severe disease [90, 91]. Tocilizumab, a monoclonal anti-IL-6-receptor blocking antibody, has been proposed as a therapeutic agent to mitigate hyperinflammation associated with COVID-19. Tocilizumab is FDA-approved for various rheumatologic conditions as well as cytokine release syndrome associated with CAR-T cell therapy.
Sarilumab, another IL-6 receptor antagonist, is currently FDA-approved for rheumatoid arthritis. Sarilumab has been used in open-label cohort studies for the management of severe COVID-19 and has undergone evaluation in unpublished RCTs for moderate and severe COVID-19 [92-96].
Summary of the evidence
Our search identified eight RCTs (including pre-prints) that reported on patients with severe COVID-19 randomized to treatment with tocilizumab (8 mg/kg) or placebo/usual care [97-104]. Gordon 2020, Horby 2021, Rosas 2020, and Veiga 2021 allowed for patients to be on mechanical ventilation at randomization, whereas the other trials included patients with a lower disease severity (e.g., allowed supplemental oxygen but excluded those on higher levels of oxygen support) or included patients with severe COVID with an inflammatory phenotype.
One trial, RECOVERY, contributed the majority of the weight in the analysis [99]. RECOVERY trial participants must have demonstrated clinical evidence of progressive COVID-19, which was defined as <92% oxygen saturation on room air or receiving oxygen and CRP ≥75 mg/L. Use of steroids was balanced across both the participants receiving tocilizumab or not receiving tocilizumab. Following recommendations for treatment with glucocorticoids, 82% of participants in both arms received dexamethasone. While RECOVERY did not blind participants or healthcare personnel to the treatment arm randomized to, this likely would not introduce bias in the objective measurement of the outcome of mortality; however, was considered as a risk of bias consideration for the more subjectively measured outcomes, clinical deterioration, along with the total body of evidence contributing to those outcomes (Table 7). There is limited safety data in the preliminary report.
Both RECOVERY and REMAP CAP (the two tocilizumab trials that reported a benefit) initiated treatment early (randomization at median of two days of hospitalization in RECOVERY; <24 hours in the ICU for REMAP-CAP), suggesting tocilizumab may be more beneficial in people with early rapidly progressive disease.
Benefits
Among hospitalized patients, tocilizumab showed a trend toward reduced mortality at 28 days compared to no tocilizumab treatment (RR: 0.91; 95% CI: 0.79, 1.04); moderate CoE). Tocilizumab demonstrated a lower relative risk of clinical deterioration, defined as death, need for mechanical ventilation, ECMO, or ICU admission, compared to placebo/usual care, RR: 0.83 (0.77, 0.89; moderate CoE). Four studies were not blinded, while healthcare personnel and outcome assessors were blinded in the remaining three trials. The panel noted that tocilizumab causes reduction in CRP levels, which would reveal the treatment arm designations of the patients, therefore introducing bias for the more subjectively measured outcomes of clinical deterioration and serious adverse events.
Harms
Serious adverse events among patients receiving tocilizumab did not differ from those not receiving tocilizumab (RR: 0.89; 95% CI: 0.74, 1.07; low CoE). An additional trial attributed treatment with tocilizumab to three serious adverse events; however, did not report events among patients not receiving tocilizumab [99]. Previously, tocilizumab has been associated with gastrointestinal perforations in non-COVID-19 settings, and case reports of bowel perforations have recently emerged with the use of tocilizumab for COVID-19 [105-108]. Increased infection risks have been noted in uncontrolled studies, and it is possible that this risk may be compounded by the combination of glucocorticoids and tocilizumab. [109, 110].
Other considerations
While the overall certainty of evidence for the trend toward a reduction in mortality was moderate, the panel believes that differences in mortality rates across the trials may be the result of the differences in baseline severity of study participants and timing of tocilizumab receipt in the disease course. In REMAP-CAP, tocilizumab was administered within 24 hours of participants’ initiating organ support in an intensive care unit, raising the possibility that this may be the optimal time to administer the drug. In RECOVERY, tocilizumab was administered to participants with oxygen saturation <92% on room air or receiving oxygen therapy, and CRP ≥75 mg/L. Given the reduction in clinical deterioration and trend toward mortality reduction, the guideline panel made a conditional recommendation for treatment of adults with tocilizumab.
The use of tocilizumab, as with other therapeutic agents that can suppress the immune system, presents additional considerations and potential concerns when used in immunocompromised hosts. The panel did not conduct an analysis of available data to assess differences in efficacy and/or adverse effects of tocilizumab among oncology or other immunocompromised patients at this time.
Conclusions and research needs for this recommendation
The guideline panel suggests tocilizumab for hospitalized adults with COVID-19.
Additional research is needed to understand the efficacy of tocilizumab when taken at different times during the course of disease. For example, there are no data to guide recommendations in patient <18 years old at this time. In addition, future studies are needed to inform the generalizability of tocilizumab with different IL-6 receptor inhibitors for patients with COVID-19 (Table s2). At the time of update, preliminary data from a trial of treatment with sarilumab has been shared as a pre-print [97]; however, number of patients who received sarilumab is limited (n=45) and the published manuscript was not available for analysis or inclusion to inform this recommendation. Other studies of sarilumab have not been made available.
Supplementary Information
Study Characteristics Table:
Forrest Plots:
- Figure s4a. Outcome of mortality for tocilizumab vs. no tocilizumab
- Figure s4b. Outcome of mortality for tocilizumab vs. no tocilizumab (sensitivity analysis for patients on mechanical ventilation for < 24 hours)
- Figure s4c. Outcome of clinical deterioration for tocilizumab vs. no tocilizumab
- Figure s4d. Outcome of severe adverse events for tocilizumab vs. no tocilizumab
Risk of Bias Table:
Recommendations 8-9: Convalescent plasma
Section last reviewed and updated 4/7/2021
Last literature search conducted 3/21/2021
Recommendation 8: Among patients hospitalized with COVID-19, the IDSA guideline panel suggests against COVID-19 convalescent plasma. (Conditional recommendation, Low certainty of evidence)
Recommendation 9: Among ambulatory patients with mild-to-moderate COVID-19, the IDSA guideline panel recommends COVID-19 convalescent plasma only in the context of a clinical trial. (Knowledge gap)
Why is convalescent plasma considered for treatment?
Convalescent plasma has been used as passive immunotherapy for prevention and treatment of infections for over 100 years [111, 112]. The predominant proposed protective mechanism is thought to be pathogen neutralization, although antibody dependent cellular cytotoxicity and enhanced phagocytosis may also play a role. With the advent of effective antimicrobial therapy (i.e., “the antibiotic era”) convalescent plasma fell out of favor. In recent years, interest in this approach has been revived as a means of addressing viral epidemics such as Ebola, SARS -1 and MERS. Studies of convalescent plasma derived from people who had recovered from those specific infections showed encouraging results, but were typically small, non-randomized, and largely descriptive [113-115]. In the current pandemic, convalescent plasma obtained from individuals who recovered from COVID-19 has been used in over 75,000 patients with moderate to severe infection as part of an expanded access program [116]. When measurement of neutralizing antibody titers is available, the FDA recommends neutralizing antibody titers of at least 1:160. Assays to measure neutralizing antibody titers were not widely available early in the pandemic so it is unclear if the plasma used in the context of the expanded access program had adequate titers of neutralizing antibodies meeting the FDA targets. Multiple prospective clinical trials are in progress utilizing plasma with an IgG enzyme-linked immunosorbent assay (ELISA) titer cutoff of ≥1:320. Titers at that level are seen in about 80% of donors [117]. The probability of obtaining a neutralizing antibody titer of ≥1:160 is highest (80% or greater) when the ELISA IgG titer is ≥1:1,350 [118]. In an analysis of the convalescent plasma expanded access program, higher levels of antibodies were associated with significant improvements in mortality compared to those receiving convalescent plasma with lower concentrations of neutralizing antibodies [116]. Regarding timing of treatment: Based on historical experience and emerging data, efficacy appears best when convalescent plasma is given at earlier stages of the disease and particularly prior to when patients become critically ill [119, 120]. The analysis of the convalescent plasma expanded access program suggests the most benefit is seen when convalescent plasma is given in the first three days from diagnosis [116]. In August 2020, the FDA issued an emergency use authorization (EUA) for investigational convalescent plasma for the treatment of COVID-19 in hospitalized patients [121]. In early February 2021, the FDA issued a revision to the EUA to limit the authorization to the use of high-titer COVID-19 convalescent plasma for the treatment of hospitalized patients early in the disease course [122].
Summary of the evidence
Our search identified and was informed by evidence from eleven RCTs and a large (n=20,000), single-arm registry study [111-115, 117-120, 123-125], as they provided the best available evidence for the outcomes of mortality, need for mechanical ventilation, serious adverse events, and adverse events. Ten of those RCTs reported on convalescent plasma transfusions for patients hospitalized with COVID-19 (Table 8) [111-114, 117-120, 123, 124] and one RCT reported on receipt of convalescent plasma by ambulatory persons with mild COVID-19 disease (Table 9) [115].
Ten trials randomized 13,026 patients hospitalized with COVID-19 to receive a transfusion with COVID-19 convalescent plasma [111-114, 117-120, 123, 124]. Several trials were open-label and/or had concerns with risk of bias due to lack of adjustment for critical confounders or potential for residual confounding (Table s12a). Timing of receipt of COVID-19 convalescent plasma during the clinical course of the patients’ illness varied across studies (Table s11). One trial reported on 160 persons who received high-titer convalescent plasma less than 72 hours after the onset of symptoms of COVID-19 (mean age: 77.2 years; standard deviation: ±8.6 years) [115]. In addition, Joyner 2020 reported on safety outcomes of over 20,000 patients enrolled in the same FDA Expanded Access Program for COVID-19 convalescent plasma study.
Benefits
Hospitalized patients
Convalescent plasma transfusion failed to show or to exclude a beneficial or detrimental effect on mortality based on the body of evidence from RCTs (RR: 0.86; 95% CI: 0.69, 1.06; moderate CoE). Receipt of COVID-19 convalescent plasma may not reduce the need for mechanical ventilation (RR: 1.11; 95% CI: 0.95, 1.30; low CoE); however, the evidence is uncertain because of concerns with risk of bias and fragility of the estimate due to small number of events reported.
Ambulatory persons
Receipt of COVID-19 convalescent plasma may reduce progression to severe respiratory disease (RR: 0.52; 95% CI: 0.29, 0.94; low CoE); however, the evidence is uncertain, as oxygenation and respiration rates are surrogate measures of need for ventilation, morbidity, and death, and because of the fragility of the estimate due to small number of events reported. Convalescent plasma transfusion may reduce mortality and clinical deterioration based on the body of evidence from an RCT (RR: 0.50; 95% CI: 0.09, 2.65; low CoE and RR: 0.58; 95% CI: 0.24, 1.40; very low CoE, respectively); however, the evidence is uncertain due to concerns with fragility of the estimate due to small number of events reported and the wide confidence interval failing to exclude a beneficial or detrimental effect.
Harms
In the largest safety study (n=20,000), within four hours of completion of convalescent plasma transfusion authors reported 146 serious adverse events classified as transfusion reactions (<1% of all transfusions) [125]. Of these, 63 deaths were reported (0.3%), 13 judged as possibly or probably related to the transfusion. The non-mortality serious adverse events include 37 reports of transfusion-associated circulatory overload, 20 cases of transfusion-related acute lung injury, and 26 cases of severe allergic transfusion reactions.
Within seven days of transfusion, 1,711 deaths were reported (mortality rate: 8.56%; 95% CI: 8.18, 8.95). In addition, 1,136 serious adverse events were reported: 643 cardiac events (569 judged as unrelated to the transfusion), 406 sustained hypotensive events requiring intravenous pressor support, and 87 thromboembolic or thrombotic events (55 judged as unrelated to the transfusion).
Four trials among patients hospitalized for COVID-19 could not exclude an increase in mild-to-severe adverse events among patients receiving convalescent plasma (RR: 1.02; 95% CI: 0.64, 1.62; low CoE) [113, 114, 118, 120]; however, the evidence was uncertain due to concerns with lack of blinding. In addition, included studies lacked a standard definition for what met the definition of an adverse event. One trial conducted among ambulatory persons receiving early, high-titer convalescent plasma did not report any serious adverse events [115].
Other considerations
Hospitalized patients
The panel agreed that the overall certainty of evidence is low due to concerns with risk of bias and imprecision. The guideline panel recognized the inability to exclude a meaningful beneficial or detrimental effect of convalescent plasma transfusion on mortality from the existing large body of evidence.
Ambulatory persons
The panel agreed that the overall certainty of evidence is low due to concerns with risk of bias and imprecision, which recognized the limited events and concerns with fragility. The guideline panel recognized the uncertainty of potential benefit when high titer convalescent plasma is given early in the course of COVID-19 disease.
Conclusions and research needs for this recommendation
The guideline panel suggests against COVID-19 convalescent plasma for persons hospitalized with COVID-19. The guideline panel recommends COVID-19 convalescent plasma for ambulatory persons only in the context of a clinical trial. Additional clinical trials are needed to determine whether there is a benefit of treatment with COVID-19 convalescent plasma and at what dose (neutralizing antibody titers), especially for patients early in the disease course of COVID-19 (Table s2). Existing data suggests that if a benefit exists, convalescent plasma is most useful when given early and with a high titer of neutralizing antibodies; future trials should attempt to compare outcomes of convalescent plasma given in this optimal setting to the standard of care. Additional research is needed to determine if different treatment effects are reported based on the severity of disease, and timing in the disease course. In addition, it is important to identify its efficacy in unique sub-populations like patients with diseases or therapies that cause immunoglobulin deficiencies.
Supplementary Information
Study Characteristics Table:
Forrest Plots:
- Figure s5a. Forest plot for the outcome of mortality for convalescent plasma vs. no convalescent plasma
- Figure s5b. Forest plot for the outcome of mechanical ventilation for convalescent plasma vs. no convalescent plasma
- Figure s5c. Forest plot for the outcome of adverse events (mild-to-severe) for convalescent plasma vs. no convalescent plasma
Risk of Bias Tables:
- Table s12a. RCTs (convalescent plasma vs. no convalescent plasma)
- Table s12b. Non-randomized studies (convalescent plasma vs. no convalescent plasma)
Recommendations 10-12: Remdesivir
Section last reviewed and updated 5/16/2021
Last literature search conducted 4/30/2022
Recommendation 10a: In hospitalized patients with severe* COVID-19, the IDSA panel suggests remdesivir over no antiviral treatment. (Conditional recommendation, Moderate certainty of evidence)
*Severe illness is defined as patients with SpO2 ≤94% on room air.
Recommendation 10b: In patients with COVID-19 on invasive ventilation and/or ECMO, the IDSA panel suggests against the routine initiation of remdesivir (Conditional recommendation, Very low certainty of evidence)
Recommendation 11: In patients on supplemental oxygen but not on mechanical ventilation or ECMO, the IDSA panel suggests treatment with five days of remdesivir rather than 10 days of remdesivir. (Conditional recommendation, Low certainty of evidence)
Recommendation 12: In patients with COVID-19 admitted to the hospital without the need for supplemental oxygen and oxygen saturation >94% on room air, the IDSA panel suggests against the routine use of remdesivir. (Conditional recommendation, Very low certainty of evidence)
Why is remdesivir considered for treatment?
Remdesivir (GS-5734) is an antiviral drug with potent in vitro activity against a range of RNA viruses including MERS-CoV, SARS-CoV 1 & 2 [126-128]. Remdesivir acts by causing premature termination of viral RNA transcription [128]. Its use improved disease outcomes and reduced viral loads in SARS-CoV-1 infected mice [127]. In rhesus macaques, therapeutic treatment with remdesivir showed reduction in SARS-CoV-2 loads, pathologic changes, and progression of clinical disease [129]. In this same animal model, remdesivir treatment initiated 12 hours post-inoculation reduced clinical signs, virus replication in the lungs, and decreased the presence and severity of lung lesions.
Summary of the evidence
Hospitalized patients with oxygen saturation >94% without supplemental oxygen
Three RCTs compared treatment with five days of remdesivir (200 mg day one, 100 mg daily days 2-5), 10 days of remdesivir (200 mg day one, 100 mg daily days 2-10), or no remdesivir for patients hospitalized with oxygen saturation >94% on room air [32, 130, 131] (Table 10a). The outcomes assessed were mortality, clinical improvement, and serious adverse events. Adaptive Covid-19 Treatment Trial (ACTT-1) and SOLIDARITY provided subgroup analyses among patients with mild-to-moderate disease [32, 130]. Randomization and lack of blinding failed to control for or balance receipt of co-interventions (e.g., treatment with dexamethasone, tocilizumab, hydroxychloroquine, and lopinavir/ritonavir) equally across arms in Spinner et al (2020) [131]. In addition, the Spinner et al did not adjust for severity of disease.
Hospitalized patients with SpO2 ≤94% on room air
Three RCTs comparing treatment with remdesivir (200 mg day one, 100 mg daily days 2-10) against no remdesivir treatment [32, 130, 132], and one RCT comparing five days of treatment (200 mg day one, 100 mg daily days 2-5) against 10 days (200 mg day one, 100 mg daily days 2-10) of treatment [133] served as the best available evidence among hospitalized persons with severe COVID-19 (Table 10b, Table 11, and Table 12). The outcomes assessed were mortality, time to clinical improvement, need for mechanical ventilation, serious adverse events, and adverse events leading to treatment discontinuation.
All trials used different definitions of severe disease for participants. ACTT-1 participants were considered to have severe disease if they required mechanical ventilation, supplemental oxygen, if SpO2 was 94% or lower while breathing ambient air, or if they had tachypnea (respiratory rate >24 breaths per minute) [130]. Within the SOLIDARITY trial (available only as a pre-print at this time), participants with severe disease were receiving mechanical ventilation [32]. In Wang 2020, severe participants had a SpO2 <94% while breathing room air or a ratio of arterial oxygen partial pressure to fractional inspired O2 of <300 mm Hg and radiologically confirmed pneumonia.
Updated analyses include the final analysis from the ACTT-1 and the interim analysis of the SOLIDARITY trial [32, 130]. SOLIDARITY reported mortality among persons remaining in hospital up to the duration of the study; however, among patients discharged before the end of the study, mortality may not have been collected completely. The study by Wang et al (2020) was stopped early due to lack of recruitment into the trial due to decreased incidence in China.
Randomization performed in Goldman 2020 failed to establish prognostic balance between baseline clinical status among the 397 patients randomized into the treatment arms, with patients in the 10-day arm more severely ill at study entry. Even with the adjusted analysis, residual confounding is possible. In addition, participants, healthcare workers, and outcome assessors were not blinded to the treatment arms.
Hospitalized patients on invasive ventiliation and/or ECMO
Subgroups from SOLIDARITY and ACTT-1 reported on the outcomes of mortality, time to recovery and serious adverse events among patients on invasive ventilation or ECMO [32, 130] (Table 10b). The duration of ventilation at time of treatment with remdesivir was not reported in ACTT-1. This may introduce uncertainty when assessing outcomes of mortality or time to recovery.
In ACTT-1 [130], randomization was stratified by study site and disease severity at enrollment. Disease severity groups were mild-moderate COVID-19 (SpO2 > 94%) and severe COVID-19 (SpO2 ≤ 94%). The severe COVID-19 stratum included patients who were hypoxemic with various degrees of severity including those requiring low flow oxygen by nasal cannula, those needing high flow oxygen, non-invasive ventilation, invasive mechanical ventilation and ECMO. In addition to analyses on established strata, authors performed post hoc analyses for subgroups within the strata (e.g., receiving oxygen, receiving high-flow oxygen or noninvasive mechanical ventilation, or receiving mechanical ventilation or ECMO), which may introduce concerns with risk of bias and imprecision when making inferences on efficacy of remdesivir among these subgroups including mechanically ventilated patients.
Benefits
Hospitalized patients with oxygen saturation >94% without supplemental oxygen
Treatment with a five- or ten-day course of remdesivir failed to show or to exclude a reduction in mortality when compared with no remdesivir (RR: 0.69; 95% CI: 0.36, 1.34; Very low CoE). A five-day course of remdesivir may increase clinical improvement over no remdesivir (RR: 1.16; 95% CI: 1.00, 1.34; Very low CoE) but a 10-day course of remdesivir was not associated with improved clinical status as compared with no remdesivir. Patients with mild-to-moderate disease receiving treatment with remdesivir had similar median time to recovery (median 5 vs. 5 days; Rate ratio: 1.22; 95% CI: 0.82, 1.81; Very low CoE).
Hospitalized patients with SpO2 ≤94% on room air
The pooled analysis failed to show a mortality benefit at 28 days (RR: 0.92; 95% CI: 0.77, 1.10; Low CoE) [32, 130, 132]. Patients receiving treatment with remdesivir trend toward greater clinical improvement at 28 days than patients not receiving remdesivir (RR: 1.13; 95% CI: 0.91, 1.41; Low CoE) [132]. In addition, based on a post-hoc analysis of patients with severe COVID-19, receiving treatment with remdesivir had a shorter median time to recovery (median 11 vs. 18 days; Rate ratio: 1.31; 95% CI: 1.12, 1.52; Low CoE) and decreased need for mechanical ventilation (RR: 0.57; 95% CI: 0.42, 0.79; Moderate CoE) [130].
In the study by Goldman et al that compared five and ten days of treatment, the shorter course of remdesivir showed a trend toward decreased mortality (RR: 0.75; 95% CI: 0.51, 1.12; Low CoE) and increased clinical improvement at 14 days (RR: 1.19; 95% CI: 1.01, 1.40; Low CoE); however, the evidence is uncertain because the persons in the 10-day group had more severe disease at baseline and there is the possibility of residual confounding despite the adjusted analysis [133].
Hospitalized patients on invasive ventilation and/or ECMO
Treatment with remdesivir failed to show a reduction in mortality (RR: 1.23; 95% CI: 0.99, 1.53; Low CoE). Similarly, remdesivir failed to show or exclude a reduction in time to recovery among patients on invasive ventilation and/or ECMO (HR: 0.98; 95% CI: 0.70, 1.36; Very low CoE).
Harms
Hospitalized patients with oxygen saturation >94% without supplemental oxygen
Patients treated with five days of remdesivir do not appear to experience greater serious adverse events than those not receiving remdesivir (RR: 0.64; 95% CI: 0.31, 1.31; Very low CoE).
Hospitalized patients with SpO2 ≤94% on room air, including patients on supplemental oxygen, on mechanical ventilation and ECMO
Patients treated with remdesivir do not appear to experience greater SAEs (grade 3/4) than those not receiving remdesivir (RR: 0.87; 95% CI: 0.59, 1.28; Moderate CoE) [130, 132].
Patients receiving five days of remdesivir may experience fewer SAEs and AEs leading to treatment discontinuation than patients receiving 10 days of remdesivir (RR: 0.61; 0.44, 0.85; Low CoE and RR: 0.44; 95% CI: 0.21, 0.95; Low CoE, respectively); however, this evidence is uncertain because of the increased severity of disease among patients in the 10-day arm [133].
Hospitalized patients on invasive ventilation and/or ECMO
Patients on invasive ventilation and/or ECMO treated with remdesivir do not appear to experience greater serious adverse events than those not receiving remdesivir (RR: 0.79; 95% CI: 0.54, 1.16; Moderate CoE).
Other considerations
Hospitalized patients with oxygen saturation >94% without supplemental oxygen
The panel agreed that the overall certainty of the evidence for treatment of patients with an oxygen saturation >94% with remdesivir compared to no remdesivir was very low due to concerns with study limitations and imprecision. Because of the study limitations and the relatively small effect of remdesivir in patients with moderate COVID-19, the panel suggests remdesivir not be used routinely in these patients. There is a need for more rigorous trials to assess the benefits and harms of remdesivir in patients with moderate COVID-19.
Hospitalized patients with SpO2 ≤94% on room air
The panel agreed that the overall certainty of the evidence for treatment of persons with severe disease with remdesivir compared to no remdesivir treatment was moderate due to concerns with imprecision. Given the inconsistent definition used in the evidence to describe baseline severity, the panel recognized a knowledge gap when assessing whether greater benefit could be attained for patients with oxygen saturation >94% and no supplemental oxygen; however, they agreed that the reported data supported the prioritization of remdesivir among persons with severe but not critical COVID-19.
The panel agreed on the overall certainty of the evidence for treatment with a five-day course compared to a 10-day course of treatment as low due to concerns with risk of bias and imprecision. The panel recognized the benefit of a shorter course of treatment, if providing similar or greater efficacy, on the availability of remdesivir. However, in a subgroup analysis of mechanically ventilated patients, the duration of treatment was 10 days in ACCT-1 trial; therefore, the panel recognized that a longer course of treatment could be desirable in this population.
Hospitalized patients on invasive ventilation and/or ECMO
The panel agreed on the overall certainty of the evidence for treatment of patients on invasive ventilation and/or ECMO with remdesivir as very low due to concerns with risk of bias and imprecision. The panel recognized that the estimates of effect for mortality and time to recovery exclude almost any benefit.
Pediatric use
There are no randomized controlled data assessing efficacy of remdesivir for treatment of hospitalized pediatric patients with COVID-19. A report of 77 children who received remdesivir through compassionate use early in the pandemic found good tolerability in this population with a low rate of serious adverse events [134].
An ongoing study of remdesivir in children [135] is using 5 mg/kg on day one (maximum dose 200 mg) followed by 2.5 mg/kg daily in patients over 14 days of age, gestational age more than 37 weeks, and weight greater than or equal to 2.5 kg. The FDA EUA applies to patients weighing over 3.5 kg and applies to the lyophilized powder formulation only.
Conclusions and research needs for this recommendation
The guideline panel suggests against remdesivir for routine treatment of patients with oxygen saturation >94% and no supplemental oxygen; however, strongly urges continued study through recruitment into RCTs.
The guideline panel suggests remdesivir rather than no remdesivir for treatment of severe COVID-19 in hospitalized patients with SpO2 <94% on room air. However, the guideline panel suggests against the routine initiation of remdesivir among patients on invasive ventilation and/or ECMO. Additional clinical trials are needed to provide increased certainty about the potential for both benefit and harms of treatment with remdesivir, as well as to understand the benefit of treatment based on disease severity.
Prescribing information in the United States recommends against use of remdesivir in patients with estimated glomerular filtration rate less than 30 mL per minute. This recommendation arises from concern about accumulation of the excipient (betadex sulfobutyl ether sodium) in such patients with potential for hepatic and renal toxicity due to that substance. Additional research into safety of remdesivir in patients with reduced renal function is needed to ascertain whether this concern is substantiated.
Immunocompromised patients who are unable to control viral replication may still benefit from remdesivir despite SpO2 that exceeds 94% on room air or a requirement for mechanical ventilation. Management of immunocompromised patients with uncontrolled viral replication is a knowledge gap and additional research into such populations is needed.
In addition, research is needed to address gaps in the evidence of effectiveness of remdesivir based on vial load.






Supplementary Information
Study Characteristics Table:
Risk of Bias Table:
Recommendation 13: Famotidine
Section last reviewed and updated 6/22/2020
Last literature search conducted 6/18/2020
Recommendation 13: Among hospitalized patients with severe COVID-19, the IDSA panel suggests against famotidine use for the sole purpose of treating COVID-19 outside of the context of a clinical trial. (Conditional recommendation, very low certainty of evidence)
The last literature search was conducted on June 18, 2020 and we identified one non-randomized study in OVID. There were no new non-indexed RCTs available.
Why is famotidine considered for treatment?
Anecdotal reports from China suggest that patients infected with coronavirus who were receiving famotidine, a H2 receptor antagonist to treat conditions such as acid reflux and peptic ulcer disease, had improved survival vs. those receiving proton pump inhibitors (PPIs) [136]. This post hoc finding summarized below has led to interest in the drug, though no predominant theory describing a mechanism for its efficacy yet exists. One theory is that famotidine, like many other compounds, binds and therefore inhibits the coronavirus main protease, 3C-like main protease (3CLpro) [137].
Summary of the evidence
Our search identified one cohort study that compared 84 patients treated with famotidine against 1,536 patients not receiving treatment with famotidine [138] (Table 13). Fifteen percent of patients in the famotidine group (13/84) started famotidine at home before presenting to the hospital. In addition, a subset of 420 patients not treated with famotidine were matched on baseline characteristics to the treated patients.
Benefits
Famotidine may decrease the composite outcome of death or intubation (HR: 0.42; 95% CI: 0.21, 0.85; Very low CoE); however, the evidence is very uncertain (Table 13).
Harms
Famotidine is well tolerated. Common adverse events include diarrhea or constipation but occur in less than 5% of people. Severe adverse events occur in less than 1% of persons taking famotidine.
Other considerations
The panel determined that the certainty of evidence to be very low due to concerns with risk of bias, imprecision, and possible publication bias. The panel agreed that critically ill patients (i.e., mechanically ventilated) may have been more likely to receive PPIs than famotidine, thus potentially allocating more prognostically favorable patients to the famotidine group; however, the study did not report a protective effect associated with the use of PPIs.
Conclusions and research needs for this recommendation
The guideline panel suggests against famotidine for the sole purpose of treating COVID-19, unless in the context of a clinical trial. Additional clinical trials are needed to inform research for treatment with famotidine for patients with COVID-19 (Table s2).
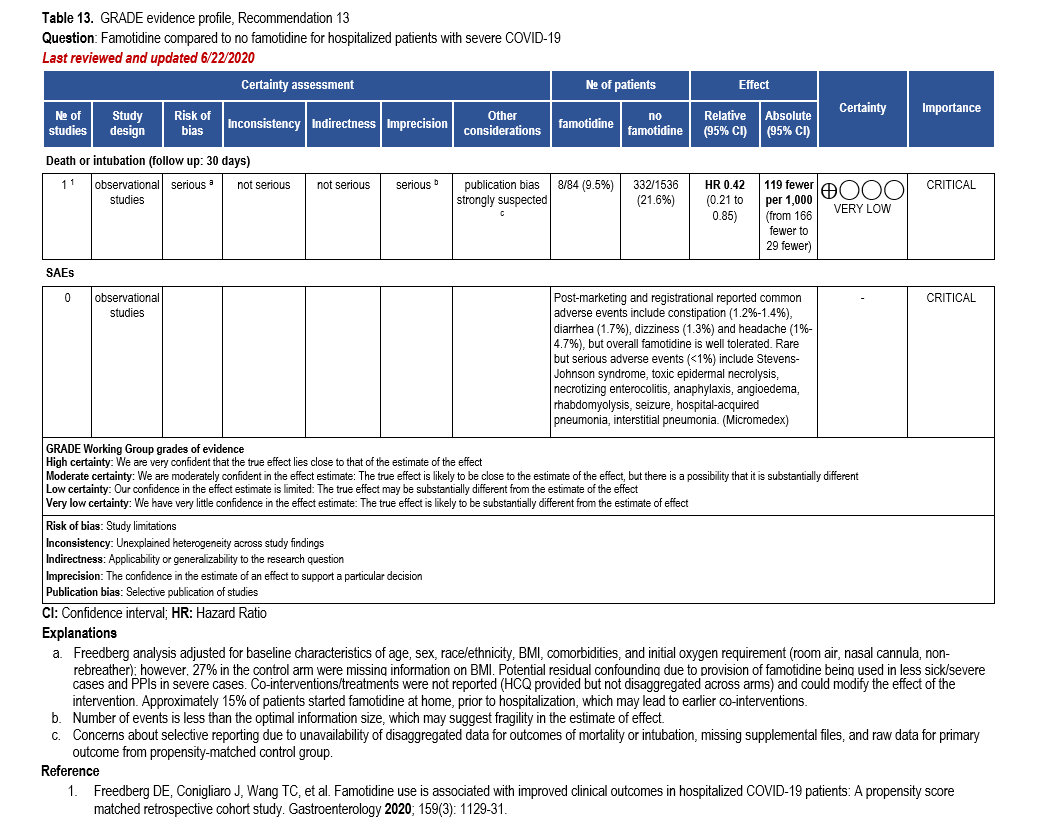
Supplementary Information
Study Characteristics Table:
Risk of Bias Table:
Recommendation 14-15: SARS-CoV-2 neutralizing antibodies
Section last reviewed and updated 4/11/2021
Last literature search conducted 3/31/2021
Recommendation 14: Among ambulatory patients with mild to moderate COVID-19 at high risk for progression to severe disease, the IDSA guideline panel suggests bamlanivimab/etesevimab or casirivimab/imdevimab rather than no neutralizing antibodies. (Conditional recommendation, low certainty of evidence)
- Remarks:
- Patients with mild to moderate COVID-19 who are at high risk of progression to severe disease admitted to the hospital for reasons other than COVID-19 may also receive bamlanivimab/etesevimab or casirivimab/imdevimab.
- Local variant susceptibility may be considered in the choice of the most appropriate neutralizing antibody therapy.
- There are limited data on efficacy of bamlanivimab/etesevimab or casirivimab/imdevimab in high-risk patients between 12 and 18 years of age.
Recommendation 15: Among hospitalized patients with severe COVID-19, the IDSA guideline panel recommends against bamlanivimab monotherapy. (Strong recommendation, Moderate certainty of evidence)
Reference
- U.S. Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency Use Authorization (EUA) of Bamlanivimab and Etesevimab. Available at: https://www.fda.gov/media/145802/download. Accessed 9 April 2021.
- U.S. Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency Use Authorization (EUA) of Casirivimab and Imdevimab. Available at: https://www.fda.gov/media/143892/download. Accessed 9 April 2021.
Why are neutralizing antibodies considered for treatment?
Neutralizing antibodies directed at the receptor-binding domain of SARS-CoV-2 spike protein have been evaluated as prophylactic and therapeutic agents for COVID-19. In animal models, there is evidence that antibody therapy may more rapidly reduce viral load in the upper and lower airways of infected animals resulting in reduced viral-induced pathology [139]. Additionally, antibody mediated enhancement of disease has not been detected in animal models [139] but this potential phenomenon should be closely monitored in the future studies.
Potential advantages of neutralizing antibodies include the ability to standardize the amount of neutralizing activity and the possibility of conferring protection more rapidly than with vaccine-induced immune responses (which generally take several weeks).
Antibody treatments have been and continue to be evaluated in both hospitalized and ambulatory patients. For outpatients, logistical challenges exist since the infrastructure for administration of intravenous (IV) infusions does not exist in most ambulatory care settings. There may also be concerns about spread of contagion when administering IV infusions in clinics. However, these challenges are being addressed in a number of outpatient infusion centers.
As of the end of February 2021, the FDA has released three emergency use authorizations for neutralizing monoclonal antibody therapies. On November 9, 2020, the FDA released an emergency use authorization for bamlanivimab [140], on November 21, 2020 for the combination of casirivimab and imdevimab [141], and on February 9, 2021 for bamlanivimab and etesevimab [142].
Summary of the evidence
Our search identified four RCTs reporting on treatment with neutralizing antibodies (bamlanivimab or combination of casirivimab/imdevimab or bamlanivimab/etesevimab) for patients with COVID-19 [143-147] (Table 14, Table 15, and Table 16). Due to clinical heterogeneity of the outcome measures across studies, meta-analyses combining the different neutralizing antibodies was not considered appropriate. One RCT, stopped early for futility, reported on hospitalized patients with COVID-19 randomized to treatment with either a single infusion of bamlanivimab (7000 mg) or placebo (ACTIV-3/TICO) [146, 147]. One Phase II/III RCT reported on non-hospitalized patients (adults as well as children age 12 and up) considered at high risk for progression to severe disease who were within three days of their first positive test for SARS-CoV-2 who were randomized to a single infusion of bamlanivimab 2,800 mg/etesevimab 2,800 mg or placebo [146]. One Phase II RCT reported on non-hospitalized patients with recently diagnosed mild or moderate COVID-19 randomized to treatment with either a single infusion of neutralizing antibody bamlanivimab in one of three doses (700 mg, 2800 mg, or 7000 mg) or placebo [145, 146].
A press release on the phase III trial assessing casirivimab/imdevimab in non-hospitalized patients reported that the independent data monitoring committee found both the 1200 mg and 2,400 mg dose had “clear clinical efficacy on reducing the rate of hospitalizations and death.” Data was provided from the company providing evidence on mortality, hospitalization, and serious adverse events. Data used to generate the evidence profile was from the modified full analysis set (mFAS), which included all randomized patients with a positive SARS-CoV-2 RT-qPCR from nasopharyngeal swabs at randomization and ≥1 risk factor for severe COVID-19 [148].
Benefits
Bamlanivimab/etesevimab
In ambulatory patients at high risk for severe COVID-19, bamlanivimab/etesevimab demonstrated an absolute mortality reduction of 1.9% (95% CI includes a minimum of 0.7% reduction in mortality) as no deaths were seen by day 29 in the 518 patients treated with bamlanivimab/etesevimab compared to 10 deaths in the 517 patients who received placebo. However, due to the small number of events (10, of which nine were believed to the result of COVID-19), the certainty of evidence was low due to imprecision. Bamlanivimab/etesevimab demonstrated a lower relative risk of COVID-19 related hospitalizations (defined as ≤24 hours of acute care) through day 29 compared to no bamlanivimab/etesevimab (RR: 0.30; 95% CI: 0.16, 0.59; low CoE). Ambulatory patients who received bamlanivimab/etesevimab had a lower relative risk of persistently high viral load at day seven compared to no bamlanivimab/etesevimab (RR: 0.34; 95% CI: 0.25-0.46; low CoE).
Casirivimab/imdevimab
Among ambulatory patients with at least one risk factor for severe disease, casirivimab/imdevimab demonstrated a lower relative risk of mortality compared to no casirivimab/imdevimab (RR: 0.28; 95% CI: 0.05, 1.40; moderate CoE). In ambulatory patients with at least one risk factor for severe disease, there was a lower relative risk of hospitalization in patients treated with casirivimab/imdevimab compared to no casirivimab/imdevimab (RR:0.45; CI: 0.30, 0.67; low CoE). Hospitalization was defined as a medically attended visit and included telemedicine visits, in-person visits, urgent care or emergent department visits, and hospitalization. The low certainty of evidence was due to indirectness, as hospitalization is a surrogate for mortality, and imprecision, due to few events recorded.
Bamlanivimab monotherapy
Among ambulatory patients, bamlanivimab demonstrated a lower relative risk of hospitalization, including visits to the emergency room, compared to no bamlanivimab (RR: 0.26; 95% CI: 0.09, 0.75; very low CoE). The very low certainty of evidence was due to indirectness, as the treatment may not have been provided to enough patients at risk of developing severe disease to be representative of the general population, and imprecision, due to few events recorded. Bamlanivimab may increase viral clearance at three days (mean difference: -0.49; 95% CI: -0.87, -0.11; low CoE); however, there may not be a meaningful difference at 11 days as measured by change from baseline SARS-CoV-2 viral load (mean difference: -0.22; 0.95: -0.60, 0.15; low CoE).
Among patients hospitalized for COVID-19, treatment with bamlanivimab compared to placebo failed to show or exclude a beneficial effect on mortality (HR: 2.00; 95% CI: 0.67, 5.99; moderate CoE). Clinical improvement, as defined as a decrease in a pulmonary ordinal scale, may not be meaningfully different among patients hospitalized for COVID-19 who received treatment with bamlanivimab or placebo (OR: 0.85; 0.56, 1.29; moderate CoE).
Harms
Bamlanivimab/etesevimab
Patients receiving bamlanivimab/etesevimab experienced more serious adverse events. However, this may not be meaningfully different from those receiving placebo (RR: 1.40; 95% CI: 0.45, 4.37; moderate CoE).
Casirivimab/imdevimab
Serious adverse events were less frequent among patients receiving casirivimab/imdevimab compared to those receiving placebo (RR: 0.31; 95% CI: 0.20, 0.46; low CoE).
Bamlanivimab monotherapy
Serious adverse events among ambulatory patients receiving bamlanivimab monotherapy may not be meaningfully different from those receiving placebo (RR: 0.15; 95% CI: 0.01, 3.78; low CoE). Patients receiving bamlanivimab did experience more infusion-related adverse events, including pruritus, flushing, rash, and facial swelling (RR: 1.62; 95% CI: 0.34, 7.70; low CoE).
Similarly, serious adverse events at five and 28 days among patients hospitalized for COVID-19 receiving bamlanivimab may not be meaningfully different from those receiving placebo (RR: 1.85; 95% CI: 0.34, 9.97; moderate CoE and RR: 0.93, 95% CI: 0.27, 3.14; moderate CoE, respectively). Similarly, infusion-related adverse events may not be meaningfully different between patients hospitalized for COVID-19 receiving bamlanivimab or placebo (OR: 1.64, 95% CI: 0.79, 3.44; moderate CoE).
Other considerations
Bamlanivimab/etesevimab
The panel agreed that the overall certainty of evidence for the treatment with bamlanivimab/etesevimab in ambulatory patients with COVID-19 was low due to imprecision and indirectness of outcomes (i.e., different dose recommended in the EUA when compared to the dose used in the trial; viral loads or hospitalizations are indirect markers of severity of disease and death). The guideline panel made a conditional recommendation for using bamlanivimab/etesevimab in mild to moderate COVID-19 at high risk for developing severe disease as the expected benefits likely outweigh any potential harms.
The FDA EUA for bamlanivimab/etesevimab was issued for the dosage of 700 mg instead of 2,800 mg of bamlanivimab, and 1,400 mg instead of 2,800 mg for etesevimab. Summary rationale for the lower dose is provided in the bamlanivimab/etesevimab FDA EUA FAQ stating “based on analysis of the available nonclinical, clinical, and virologic data, as well as supportive data from pharmacokinetic/pharmacodynamics modeling, the authorized dosage of 700 mg bamlanivimab and 1,400 mg of etesevimab is expected to have similar clinical effects to a dosage of 2,800 mg bamlanivimab and 2,800 mg of etesevimab used in the clinical study.” The lower dose from the EUA was not studied in the phase III trial BLAZE-1. The extrapolation that the lower dose has the same efficacy as the higher dose, based on surrogate outcomes from other study lowers certainty of evidence due to indirectness.
Casirivimab/imdevimab
The panel agreed that the overall certainty of evidence for the currently available data on the treatment with casirivimab/imdevimab for ambulatory patients with COVID-19 is low due to concerns with indirectness and imprecision due to sparseness of events.
Bamlanivimab monotherapy
The panel agreed that the overall certainty of evidence for treatment with bamlanivimab for ambulatory patients with COVID-19 is very low due to concerns with indirectness and imprecision. Though the treatment with combination bamlanivimab/etesevimab is preferred compared to bamlanivimab monotherapy due to the more robust data supporting it, the panel recognized that short-term supply constraints for bamlanivimab/etesevimab may necessitate the use of bamlanivimab monotherapy in some situations.
The panel agreed that the overall certainty of evidence for treatment with bamlanivimab for patients hospitalized for COVID-19 is moderate due to concerns with fragility in the estimate from the small number of events reported. The guideline panel made a strong recommendation against treatment with bamlanivimab for patients hospitalized for COVID-19. The panel was moderately certain that any relevant benefit (reduction in mortality or clinical improvement) could be excluded.
Conclusions and research needs for this recommendation
The guideline panel suggests using bamlanivimab/etesevimab or casirivimab/imdevimab in mild to moderate COVID-19 ambulatory patients at high risk for developing severe disease as the expected benefits likely outweigh any potential harms (Table 14, Table 15, and Table 16).
The guideline panel recommends against use of bamlanivimab for patients hospitalized for COVID-19 (Table 17).
The guideline panel recognized the need for continued research and accrual of evidence, particularly trials on patient important outcomes, existing and new neutralizing antibodies, and neutralizing antibodies for prophylaxis (Table s2).
The emergence and circulation of new SARS-CoV-2 genetic variants has been reported from the United States and other counties. The B.1.1.7 (United Kingdom [UK] origin), B.1.351 (South Africa origin), P.1 (Brazil origin), B.1.427, and B.1.429 (California origin) variants circulating in the United States are classified as variants of concern as they may have potential clinical and public health implications. The B.1.525, B1.526 (New York origin) and P.2 variants are classified as variants of interest [149].
In vitro neutralizing assays using SARS-CoV-2 or vesicular stomatitis virus-based pseudovirus showed that some of the variants had reduced susceptibility to the currently available neutralizing antibodies under the EUA, either individually or in combination. Bamlanivimab alone and the combination of bamlanivimab and etesevimab together had activity against pseudovirus expressing del69-70 + N501Y found in the B.1.1.7 variant (UK origin). Pseudovirus expressing spike protein from the B.1.351 lineage (South Africa origin) or substitutions K417N + E484K + N501Y found in this lineage had reduced susceptibility to bamlanivimab and etesevimab together of >45-fold, and pseudovirus expressing K417T + E484K + N501Y found in the P.1 lineage (Brazil origin) had reduced susceptibility to bamlanivimab and etesevimab together of >511-fold. Pseudovirus expressing spike protein from the B.1.427/B.1.429 lineages (California origin), or the L452R substitution found in this lineage, had reduced susceptibility to bamlanivimab and etesevimab together of 7.7-fold or 7.4-fold, respectively [142].
Casirivimab and imdevimab individually and together had neutralization activity against pseudovirus expressing all spike protein substitutions found in the B.1.1.7 lineage (UK origin) and against pseudovirus expressing only N501Y found in B.1.1.7 and other circulating lineages. Casivirimab and imdevimab together had neutralization activity against pseudovirus expressing all spike protein substitutions, or individual substitutions K417N, E484K or N501Y, found in the B.1.1351 lineage (South Africa origin), and against K417T+E484K, found in the P.1 lineage (Brazil origin), although casirivimab alone, but not imdevimab, had reduced activity against pseudovirus expressing K417N or E484K, as indicated above. The E484K substitution is also found in the B.1.526 lineage (New York origin). Casivirimab and imdevimab, individually and together, retained neutralization activity against the L452R substitution found in the B.1.427/B.1.429 lineages (California origin) [150].
It is not known how in vitro neutralization activity of monoclonal antibodies against psudovirus expressing spike protein substitutions or even in vitro neutralization activity against the SARS-CoV-2 variants correlate with clinical efficacy. Genotypic and phenotypic testing for variants and their correlation with patient important outcomes is being studied in clinical trials evaluating neutralizing antibodies. We still need further studies and surveillance data to understand the implications of SARS-CoV-2 variants on clinical efficacy of COVID-19 therapies.

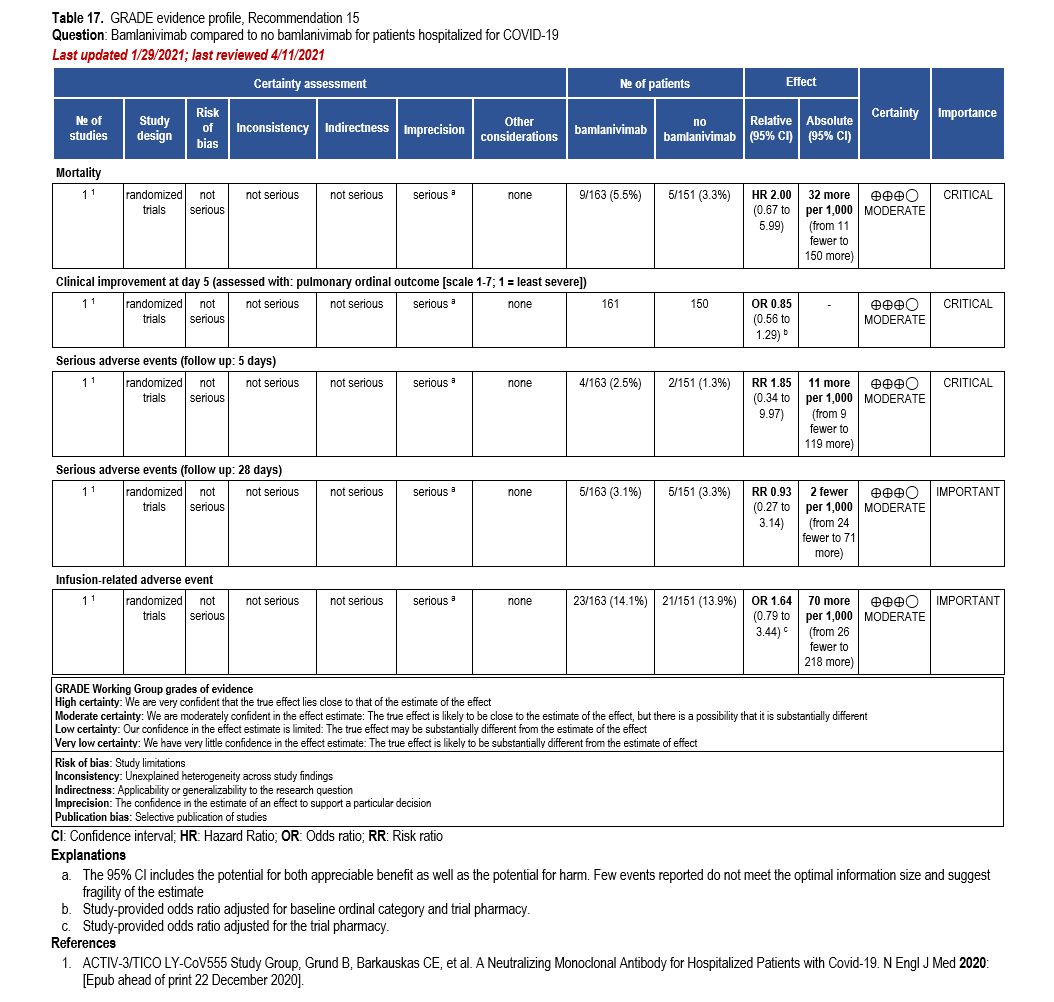
Supplementary Information
Study Characteristics Table:
- Table s17. Neutralizing antibodiesa,b,c versus no neutralizing antibodies
- Bamlanivimab/etesevimab
- Casirivimab/imdevimab
- Bamlanivimab monotherapy
Risk of Bias Table:
Recommendations 16-17: Baricitinib
Section last reviewed and updated 5/16/2021
Last literature search conducted 4/30/2021
Recommendation 16: Among hospitalized adults with severe* COVID-19 having elevated inflammatory markers but not on invasive mechanical ventilation, the IDSA panel suggests baricitinib rather than no baricitinib. (Conditional recommendation, Moderate certainty of evidence)
- Remark:
- Baricitinib 4 mg daily dose for 14 days or until discharge from hospital
- Baricitinib appears to demonstrate the most benefit in those with severe COVID-19 on high-flow oxygen/non-invasive ventilation at baseline
Recommendation 17: Among hospitalized patients with severe* COVID-19 who cannot receive a corticosteroid (which is standard of care) because of a contraindication, the IDSA guideline panel suggests use of baricitinib with remdesivir rather than remdesivir alone. (Conditional recommendation, Low certainty of evidence)
- Remark: Baricitinib 4 mg daily dose for 14 days or until hospital discharge. The benefits of baricitinib plus remdesivir for persons on mechanical ventilation are uncertain.
*Severe illness is defined as patients with SpO2 ≤94% on room air, including patients on supplemental oxygen, oxygen through a high-flow device, or non-invasive ventilation.
Why is baricitinib considered for treatment?
Baricitinib, a selective Janus kinase 1 and 2 inhibitor currently FDA-approved for the treatment of rheumatoid arthritis (RA), is being investigated in multiple studies for treatment of COVID-19. The proposed benefits of baricitinib in the management of COVID-19 may be two-fold as it has both anti-inflammatory and potential antiviral activity [151]. Janus kinase mediates cytokine signaling, which contributes to inflammation; Janus kinase inhibitors, therefore, may decrease cytokine-mediated inflammation. Baricitinib inhibits host intracellular membrane proteins AP2-associated protein kinase 1 (AAK1) and also binds cyclin G-associated kinase (GAK), both thought to play a role in receptor mediated endocytosis of many viruses including Ebola, dengue, Hepatitis C, and SARS CoV-2 [152-154]. Baricitinib has been evaluated in people with COVID-19 in both randomized and non-randomized studies [155-159].
Based on experience in clinical trials for rheumatoid arthritis, baricitinib has been found to be associated with an increased risk of adverse effects including infections (especially upper respiratory tract infections), thrombosis, lymphopenia, anemia, increases in lipids, elevations in liver enzymes, and elevations in creatinine phosphokinase [151]. Many of these side effects are thought to be dose related, with increased incidence in patients taking baricitinib 4 mg compared with 2 mg. Patients enrolled in Adaptive COVID-19 Treatment Trial (ACTT-2) and COV-BARRIER received baricitinib 4 mg daily for two weeks or until discharge, a shorter duration than those taking the drug for RA. In clinical trials for RA, baricitinib was associated with a numerically higher risk of upper respiratory tract infections and herpes simplex and herpes zoster infections compared with placebo [160]. Opportunistic infections such as herpes simplex, herpes zoster, and tuberculosis [161, 162] have been reported in patients taking baricitinib.
Patients with COVID-19 have been found to have abnormalities in coagulation parameters and might have an elevated risk of thrombosis [163]. Baricitinib has been found to increase incidence of thrombosis compared with placebo in clinical trials for its FDA approval for rheumatoid arthritis, especially at a higher dose of 4 mg daily [151]. During the 16-week treatment period in RA trials, VTE occurred in five patients treated with baricitinib 4 mg daily, compared with 0 in the 2 mg daily and placebo groups. Arterial thrombosis occurred in two patients treated with baricitinib 4 mg, two patients treated with baricitinib 2mg, and 1 patient on placebo. In ACTT-2, the percentage of patients reported to have VTE was numerically higher in the combination group (21 patients [4.1%] vs. 16 patients [3.1%]) although it was similar overall (absolute difference 1%, 95% CI -1.3 to 3.3) [164]. Of note, all patients in the trial were recommended to receive VTE prophylaxis if they had no contraindication. We do not have long-term data, especially on safety, development of the aforementioned adverse effects and opportunistic infections from these two trials.
Summary of the evidence
Baricitinib
Our literature search identified one RCT that compared the use of baricitinib (4 mg daily dose up to 14 days) to placebo in hospitalized adults with severe COVID (NIAID OS: 4 – hospitalized, not requiring supplemental oxygen; 5 – hospitalized, requiring supplemental oxygen; or 6 – hospitalized, receiving non-invasive ventilation or high-flow oxygen devices) [159]. In the COV-BARRIER trial, randomization was stratified by disease severity, age, region, and use of corticosteroids. Participants in both arms had >1 elevated inflammatory marker (CRP, d-dimer, LDH, ferritin) and also received standard of care, which included corticosteroids in 79% and/or antivirals (e.g., remdesivir in 18.9%).
Baricitinib as a steroid substitute
Our literature search identified one RCT that reported on the use of baricitinib (4 mg daily dose) plus remdesivir in hospitalized patients with moderate and severe COVID-19 ([164]. This trial was conducted as the second stage of the ACTT-2, where subjects were randomized to receive combination therapy with baricitinib and remdesivir or remdesivir alone [164] (Table 19). Randomization was stratified by disease severity classified by an OS of clinical status (4+5 vs 6+7 [7 –patients with an ordinal scale of 6 (high flow oxygen and non-invasive ventilation) or 7 (mechanical ventilation or ECMO). Mild-moderate disease was defined as patients with an ordinal scale of 4 (hospitalized, but not requiring supplemental oxygen) or 5 (requiring supplemental oxygen). The trial was initiated before corticosteroids were commonly used for severe COVID-19.
Benefits
Baricitinib
Treatment of hospitalized patients with severe COVID-19 with baricitinib rather than no baricitinib reduced 28-day mortality (HR: 0.57; 95% CI: 0.41, 0.78; Moderate CoE). The odds of COVID-19 disease progression trends toward a reduction in persons receiving treatment with baricitinib (OR: 0.85; 95% CI: 0.67, 1.08; Moderate CoE).
Baricitinib as a steroid substitute
In ACTT-2, the combination of baricitinib and remdesivir showed a trend towards lower mortality (4.7% vs. 7.1%; rate ratio: 0.65; 95% CI 0.39, 1.09; Moderate CoE). In patients stratified within the severe COVID-19 pneumonia group, defined as 6 or 7 on the ordinal scale, subjects who received baricitinib and remdesivir were more likely to experience clinical recovery (defined as a value of <4 on the ordinal scale) at day 28 (69.3% vs. 59.7%; rate ratio 1.29; 95% CI 1.00, 1.66; Moderate CoE). The original stratification was altered as 40 subjects were misclassified at baseline; however, re-analysis of the original stratified data produced a similar result. Patients in the baricitinib arm were less likely to require initiation of mechanical ventilation or ECMO through day 29 (10% vs. 15.2%; RR: 0.66; 95% CI 0.46, 0.93; Low CoE). In summary, it appeared that patients requiring supplemental oxygen or non-invasive ventilation at baseline benefitted most from baricitinib; the benefit was less clear in patients already on mechanical ventilation.
Harms
The risk of serious adverse events in patients receiving baricitinib was not greater than those not receiving baricitinib (RR: 0.82; 95% CI: 0.65, 1.03; Moderate CoE).
In ACTT-2, patients receiving baricitinib and remdesivir had a lower risk of developing any serious adverse events through day 28 (16% vs. 21%; RR 0.76; 95% CI 0.59, 0.99; Moderate CoE) whether or not thought to be related to the study drug. In this trial, the overall rate of new infections was lower in the baricitinib plus remdesivir group compared with remdesivir alone (30 patients [5.9%] versus 57 patients [11.2%]) [164]. However, patients who received concomitant glucocorticoids had a higher incidence of serious or non-serious infections as compared with those who did not: 25.1% and 5.5%, respectively. It was not specified what proportion of these patients in the study were in the baricitinib combination group versus the control group.
Other considerations
Baricitinib
The panel agreed on the overall certainty of evidence as moderate due to concerns with imprecision, as currently, only one pre-print RCT is available and some outcomes have concerns with fragility. The guideline panel recognized the resource implications based on the dose and duration reported in the trial (4 mg daily up to 14 days).
Baricitinib as a steroid substitute
The panel agreed that the overall certainty of evidence was low due to concerns with risk of bias, driven by the use of data from post-hoc analyses and imprecision, which recognized the limited events and concerns with fragility in the group who likely benefited most (those requiring supplemental oxygen or non-invasive ventilation). The guideline panel noted the importance of suggesting baricitinib plus remdesivir as an option for persons unable to receive corticosteroids.
Conclusions and research needs for this recommendation
The guideline panel suggests baricitinib in addition to standard of care for patients hospitalized with severe COVID-19. The guideline panel suggests baricitinib with remdesivir for persons for whom corticosteroids are indicated but who cannot receive them due to a contraindication. Baricitinib plus remdesivir should be reserved for patients who cannot take corticosteroids because dexamethasone has been proven to reduce mortality in patients hospitalized with COVID-19 who require supplemental oxygen or mechanical ventilation and, for this reason, dexamethasone is recommended by the panel for this group. It is uncertain whether baricitinib plus remdesivir will have the same benefit as dexamethasone. We need long term data especially 60-day mortality from COV-BARRIER study. This is particularly because despite having a reduction in 28-day mortality with baricitinib compared to placebo, there was still no statically significant difference between arms for the composite endpoint of progression to needing high flow oxygen, non-invasive & invasive mechanical ventilation, ECMO or death (Table s2). As of the time of this narrative, there were no head-to-head trials evaluating either the combination of baricitinib plus tocilizumab or evaluating baricitinib compared to tocilizumab.
Supplementary Information
Study Characteristics Table:
Risk of Bias Table:
Recommendations 18-19: Ivermectin
Section last reviewed and updated 5/28/2021
Last literature search conducted 4/30/2021
Recommendation 18: In hospitalized patients with severe COVID-19, the IDSA panel suggests against ivermectin outside of the context of a clinical trial. (Conditional recommendation, very low certainty of evidence)
Recommendation 19: In ambulatory persons with COVID-19, the IDSA panel suggests against ivermectin outside of the context of a clinical trial. (Conditional recommendation, very low certainty of evidence)
Why is ivermectin considered for treatment?
Ivermectin is an anti-parasitic agent that is FDA-approved for onchocerciasis and strongyloidiasis and is used off-label for the treatment of many parasitic infections. Although it has in vitro activity against some viruses, including SARS-CoV-2, it has no proven therapeutic utility. In vitro activity against SARS-CoV-2 [165] requires concentrations considerably higher than those achieved in human plasma and lung tissue to reach the in vitro IC50 [166]. Since ivermectin is generally well-tolerated, it was empirically evaluated in uncontrolled studies for COVID-19, alone and in combination with other off-label medications.
Summary of the evidence
Our search identified nine studies in patients with COVID-19 with ages ranging between 8 and 86 years that reported on the outcomes of mortality, symptom resolution, viral clearance, and adverse events, and informed the evidence review for inpatients and outpatients [167-178]. Eligible studies compared treatment with ivermectin against a placebo or standard of care. Studies comparing ivermectin to a non-placebo, active comparison (i.e., a different agent considered a possible treatment for COVID-19 infection by clinicians) or that did not provide a comparison arm were not included in these analyses. Several studies did not meet eligibility for inclusion in this review. Four trials compared ivermectin to hydroxychloroquine (comparison to treatment with evidence of harm) [179-182]; two trials examined ivermectin as prophylactic treatment [183, 184]; and three trials did not provide study data in a peer-reviewed, published or pre-print manuscript [182, 185, 186].
The studies that informed the recommendations for hospitalized patients included seven RCTs [167-169, 171, 172, 177, 178] and two non-randomized studies [170, 173]. Five RCTs [169, 171, 174-176] informed the recommendation for ambulatory persons. Each of them compared an active treatment arm of ivermectin to an inactive comparison (e.g., standard of care with or without placebo). Studies that compared ivermectin to other therapy (e.g., HCQ) were excluded, as the presence of a non-placebo comparator may bias the effectiveness of ivermectin.
The evidence informing the recommendations for hospitalized and ambulatory persons reported on the use of a range of doses (100 mcg/kg/day to 400 mcg/kg/day) and durations (one day up to seven days) of treatment with ivermectin. Among studies reporting on hospitalized patients, substantial heterogeneity was observed, introduced by one study (Figure s7c) [167]. Ahmed 2021 treated patients with ivermectin for a duration of five days, rather than one day as used by the remaining studies. This may explain the heterogeneity between studies; however, excluding Ahmed 2021, any meaningful reduction in viral clearance was still not demonstrated by the summary estimate (Figure s7c). Heterogeneity was not observed for other outcomes reported for hospitalized or ambulatory persons.
Among the RCTs, the risk of bias was high in two trials because of unsuccessful randomization into treatment and control groups. Hashim et al (2020) inadequately randomized participants by allocating them to respective treatment arms on odd and even days, as well as assigning all critically ill patients to the ivermectin arm, and Podder et al (2020) allocated participants based on odd or even registration numbers. In addition, across many RCTs, there were concerns due to lack of blinding of study personnel, which may lead to over- or under-estimates of treatment effects, particularly for subjective outcomes (e.g., symptom resolution, adverse events).
Benefits
Inpatients
The evidence is very uncertain, but studies suggested that ivermectin may decrease mortality among persons with COVID-19 (RR: 0.57; 95% CI: 0.36, 0.90; very low CoE). Persons receiving treatment with ivermectin rather than no ivermectin may trend toward increased symptom resolution and viral clearance (RR: 1.07; 95% CI: 0.69, 1.65; very low CoE and RR: 1.25; 95% CI: 0.72, 2.15; very low CoE, respectively).
Outpatients
The evidence is very uncertain, but ivermectin may reduce the time to recovery among outpatients with COVID-19 (mean difference: 2.02 days fewer; 95% CI: 2.16 to 1.89 days fewer; very low CoE). Similarly, the evidence is very uncertain; however, there may be a trend toward mortality reduction, avoidance of progression to severe disease, and viral clearance at day seven (RR: 0.19; 95% CI: 0.02, 1.58; very low CoE, RR: 0.44; 95% CI: 0.15, 1.26; very low CoE, and RR: 0.93; 95% CI: 0.63, 1.37; very low CoE, respectively).
Harms
In doses typically used for the treatment of parasitic infections, ivermectin is well-tolerated. We are unable to exclude the potential for adverse events in hospitalized and serious adverse events in non-hospitalized persons with COVID-19 treated with ivermectin rather than no ivermectin, (RR: 0.80; 95% CI: 0.39, 1.67; low CoE and RR: 0.99; 95% CI: 0.14, 6.96; low CoE, respectively).
Other considerations
The panel determined the certainty of evidence of treatment of ivermectin for hospitalized and non-hospitalized patients to be very low due to concerns with risk of bias (i.e., study limitations) and imprecision. In addition, there were concerns about publication bias, as the available evidence consisted mostly of positive trials of smaller size. The guideline panel made a conditional recommendation against treatment of COVID-19 with ivermectin outside of the context of a clinical trial for both patients with COVID-19 hospitalized or in the outpatient setting.
Conclusions and research needs for this recommendation
The guideline panel suggests against ivermectin for the treatment of hospitalized patients with COVID-19, unless in the context of a clinical trial. The guideline panel suggests against ivermectin for the treatment of outpatients with COVID-19, unless in the context of a clinical trial. Well-designed, adequately powered, and well-executed clinical trials are needed to inform decisions on treating COVID-19 with ivermectin (Table s2).
Supplementary Information
Study Characteristics Table:
Table s21. Ivermectin versus no ivermectin
Forrest Plots:
- Figure s7a. Outcome of mortality for ivermectin vs. no ivermectin among hospitalized patients
- Figure s7b. Outcome of viral clearance for ivermectin vs. no ivermectin among hospitalized patients (all studies)
- Figure s7c. Forest plot for the outcome of viral clearance for ivermectin vs. no ivermectin among hospitalized patients (without Ahmed)
- Figure s7d. Forest plot for the outcome of mortality for ivermectin vs. no ivermectin among ambulatory patients
- Figure s7e. Outcome of progression to severe disease for ivermectin vs. no ivermectin among ambulatory patients
- Figure s7f. Outcome of viral clearance at seven days for ivermectin vs. no ivermectin among ambulatory patients
- Figure s7g. Forest plot for the outcome of adverse events for ivermectin vs. no ivermectin among ambulatory patients
- Figure s7h. Forest plot for the outcome of time to recovery (days) for ivermectin vs. no ivermectin among ambulatory patients
Risk of Bias Tables:
- Table s22a. RCTs (ivermectin vs. no ivermectin)
- Table s22b. Non-randomized control studies (ivermectin vs. no ivermectin)
Narrative summaries of treatments undergoing evaluation
In addition to the clinical questions addressed above, the panel identified several treatments currently undergoing evaluation for which additional data are needed to rate recommendations. Narrative summaries for these treatments are provided below.
HIV antivirals
Last reviewed 4/11/2020; no updates made since 4/11/2020
In vitro antiviral activity of darunavir against SARS-CoV-2 showed no activity at clinically relevant concentrations. Three randomized, open-label clinical trials are currently listed on evaluating darunavir/cobicistat as a potential therapeutic option for COVID-19. Janssen, the manufacturer of darunavir/cobicistat has reported that one of these trials [187] has concluded that darunavir/cobicistat plus conventional treatments was not effective in achieving viral clearance at day seven post randomization, compared to conventional treatments alone. Clinical outcomes of this trial including rate of critical illness and mortality 14 days after randomization, have not been reported to date.
Lopinavir-ritonavir combined with interferon beta or other antivirals
Last reviewed and updated 9/4/2020
Lopinavir-ritonavir is a combination of protease inhibitors for the treatment of HIV infection. Lopinavir-ritonavir has been shown to have in vitro antiviral activity against beta-coronaviruses such as SARS-CoV, and MERS-CoV [59, 61, 62, 188]. Since lopinavir-ritonavir is not specifically designed for treatment of coronavirus, lopinavir-ritonavir alone may not demonstrate a difference from placebo in reducing viral load when treatment was initiated at a median of 13 days after symptoms onset [62]. In an open-label treatment trial, lopinavir-ritonavir with ribavirin reduced the mortality and requirement of intensive care support of hospitalized SARS patients compared with historical control [62]. Many interferons, especially interferon beta have been shown to have modest in-vitro antiviral activity against SARS-CoV and MERS-CoV [59, 188]. Lopinavir-ritonavir or interferon beta-1b has been shown to reduce viral load of MERS-CoV and improve lung pathology in a nonhuman primate model of common marmoset [61].
An RCT on the triple combination of lopinavir-ritonavir, ribavirin, and interferon beta-1b, compared with single agent lopinavir-ritonavir for 14 days was conducted in the treatment of 127 adult patients admitted to hospital with COVID-19 [65]. Patients who had NEWS2 of least one, and with symptom duration of 14 days or less were recruited and randomly assigned to either triple combination or control group in a ratio of 2:1. Treatment with triple combination was well tolerated, and had a significantly shorter median time to suppress the viral load in nasopharyngeal specimen, and a significantly shorter time to alleviate symptoms, and resulted in shorter hospital stay. Since the median number of days from symptom onset to the start of study treatment was five days, only one patient in the control group received ventilator support and no patient died during the study. It is not possible to generalize the effectiveness of triple therapy in critically ill patients.
Lopinavir-ritonavir was further investigated in two retrospective cohort studies using HCQ [189] and arbidol [190], an indole-derivative licensed for decades in Russia and China against influenza, for comparison. Lopinavir-ritonavir was associated with more rapid viral clearance (median, 21 days vs. 28 days) than HCQ in 65 mild to moderate COVID-19 patients in South Korea, but there was no difference in time to clinical improvement [189]. Lopinavir-ritonavir was found to be inferior to arbidol in terms of viral clearance on day 14 after admission. But the number of patients was small (n=50) and all patients received atomized inhalation of recombinant human interferon-α2b injection. The efficacy of arbidol monotherapy remains uncertain [190].
Subcutaneous injection of interferon β-1a was used for the treatment of 42 severe COVID-19 adult patients in an open-label randomized clinical trial in Iran. Although there was no significant improvement in time to clinical response in the interferon-treated group, the overall mortality at 28 days was reduced in the interferon-treated then the control group (19% vs. 43.6%, p= 0.015) [191].
COVID-19 convalescent plasma for prophylaxis
Last reviewed and updated 9/4/2020
Studies of convalescent plasma for treatment of hospitalized patients with COVID-19 were discussed in a previous section. Use of convalescent plasma as prophylaxis in individuals with high-risk exposure to SARS-CoV-2 is under study, with at least five clinical trials in clinicaltrials.gov as of August 6, 2020 that include arms in which individuals exposed to SARS-CoV-2 but without disease may receive convalescent plasma [192-196]. Issues associated with regulatory concerns, safety, workflow, and trial design were recently reviewed [197]. Distinct from the polyclonal antibodies present in convalescent plasma, monoclonal antibodies specific for respiratory viruses have also been used in certain populations for protection against disease in specific high-risk populations [198, 199], and animal models have suggested utility in prophylaxis against SARS coronavirus infection [200]. There are multiple trials listed in clinicaltrials.gov of different SARS-CoV-2 monoclonal antibodies for treatment or prophylaxis, with other potential monoclonal antibodies in earlier stages of development. No data on safety or efficacy are yet reported.
Ribavirin
Last reviewed 4/11/2020; no updates made since 4/11/2020
There are only in vitro data available on the activity of ribavirin on SARS-CoV-2 currently. The EC50 (half maximal effective concentrations) was significantly higher than for chloroquine and remdesivir, so it appears less potent in vitro compared to these agents [16]. There are limited clinical studies in SARS-CoV-1 and MERS-CoV infections. In a systematic review of ribavirin treatment in patients infected with SARS-CoV-1, 26 studies were classified as inconclusive, and four showed possible harm [201]. In a retrospective observational study in patients with MERS-CoV infection, the combination of ribavirin and interferon, compared to no antiviral treatment, was not associated with improvement in the 90-day mortality or more rapid MERS-CoV RNA clearance [202].
Oseltamivir
Last reviewed 4/11/2020; no updates made since 4/11/2020
Oseltamivir is a neuraminidase inhibitor used for prophylaxis and treatment of influenza. Given its specificity for an enzyme not found on coronaviruses, it is unclear what the mechanism of action would be against COVID-19. However, this has been used in combinations of antiviral therapy in Wuhan [203] and continues to be explored as a therapeutic option as part of combination regimens. Two trials evaluating combination regimens are underway in Wuhan [204, 205] as well as a trial in Thailand proposing different combinations [206]. None of the trials or case reports have examined oseltamivir as monotherapy.
Intravenous immunoglobulin
Last reviewed and updated 9/4/2020
Intravenous immunoglobulin (IVIg) has been used as an adjuvant to treat a variety of pathogens either as a pooled product or in a concentrated more pathogen focused (hyperimmune) form. As the community from which a given batch of IVIg is derived from includes increasing numbers of individuals who have recovered from SARS-CoV-2, the possibility of protective antibodies being present in the pooled product is increased. However, the potential utility of IVIg for the treatment of SARS-CoV-2 is unknown at this time. Its use has been reported in a few patients with COVID-19 [207], but studies are needed to determine if there may be a role for IVIg in the treatment of SARS-CoV-2.
One open-label trial randomized patients with COVID-19 (SpO2 ≤96% on ≥4 liters O2 by nasal cannula but not on mechanical ventilation) to either three days of IVIg (n=16) or no IVIg (n=17) [208]. During the study period (30 days or hospital discharge), two patients in the IVIg arm and seven in the standard of care arm required mechanical ventilation, one patient in the IVIg arm and three patients in the standard of care arm died. No adverse events were reported in the IVIg arm. Co-treatments with remdesivir, convalescent plasma, and corticosteroids were balanced across arms at baseline; however, methylprednisolone was provided with each IVIg dose in the treatment arm, and co-interventions provided during the treatment period were unbalanced. One retrospective cohort reported on 58 patients who received IVIg; however, the study did not identify a standard of care group and multiple co-treatments were provided [209]. Two case series reported on eight patients [207, 210] with severe COVID-19 who received IVIg for five consecutive days. All patients were discharged from the hospital.
Should NSAIDS be stopped in patients with COVID-19?
Last reviewed and updated 9/4/2020
The role of nonsteroidal anti-inflammatory drugs (NSAIDs) in the management of SARS-CoV-2 was debated widely in the first few months of the COVID-19 pandemic. The discussion was prompted by warnings from European health officials regarding the possibility of increased risk of infection or severity of disease in those taking NSAIDS. These concerns were based on early unconfirmed reports in four patients and supported by theoretical mechanistic concerns about the role NSAIDs play in SARS-CoV-2 pathogenesis. Human coronaviruses, including SARS-CoV-2, use ACE2 to bind to human targets and gain entry into target cells [211]. It has been theorized that NSAIDs, due to upregulation in ACE2 in human target cells, may lead to an increased risk of infection or a more severe course of COVID-19 in those taking NSAIDs. In addition, there are well known risks of non-steroidal anti-inflammatory agents including cardiovascular, gastrointestinal and renal adverse events [212, 213]. In the setting of bacterial pneumonia, NSAIDs may impair recruitment of polymorphonuclear cells, resulting in a delayed inflammatory response and resolution of infection, however a causal relationship has not been established [214, 215].
A case-control study from Italy published in May 2020 did not demonstrate an increased risk of SARS-CoV-2 infection in those taking NSAIDs chronically (adjusted OR: 1.06; 95% CI 0.98, 1.15) [216]. In April 2020, the WHO produced a scientific brief detailing a systematic review that included 73 studies in patients with acute respiratory infections. While no direct studies for patients with MERS, SARS or SARS-CoV-2 were available for analysis, there was no evidence of adverse events [217]. In a large registry trial that included data from five hospitals in Massachusetts, there was a lower risk of hospitalization in those with SARS-CoV-2 prescribed naproxen or ibuprofen, however it is difficult to determine if these patients were actively taking these medications at the time of COVID-19 diagnosis [218]. Randomized controlled trials are currently underway to better understand the safety of NSAIDs in the management of patients with COVID-19 [219, 220].
Should ACE inhibitors and ARBs for hypertension be stopped in patients with COVID-19?
Last reviewed and updated 9/4/2020
Angiotensin converting enzyme 2 (ACE2) is the entry receptor for SARS-CoV-2 on human cells. Animal experiments have shown mixed findings on the effect of angiotensin-converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARBs) on ACE2 levels and activity, leading to two contrasting hypotheses in COVID-19 [221-223]. The harmful hypothesis is that ACEIs and ARBs may increase the risk of infection and severity of COVID-19 via increased ACE2 expression. On the contrary, infection with other coronaviruses have been shown to decrease ACE2 levels in vitro [224], which may lead to increased angiotensin II activity resulting in pulmonary, cardiovascular and other end organ damage in patients with COVID-19 [221, 225]. This has led to speculation about a beneficial hypothesis that ACEI and ARBs may have a therapeutic role in COVID-19, by inhibiting the renin-angiotensin-aldosterone axis.
There have been several recent observational studies on the effects of ACEIs and ARBs in patients tested for and diagnosed with COVID1-19. A multi-center retrospective study [226] evaluated 1,128 patents admitted to nine hospitals in Hubei province, China with COVID-19 including 188 (17%), who were on an ACEI or ARB. The risk of 28-day all-cause mortality was lower in ACEI/ARB group vs non-ACEI/ARB group (IRD: -0.24; 95% CI: -0.43, -0.05). After adjusting the all-cause mortality was still lower in the ACEI/ARB group compared to the non-ACEI/ARB group (HR: 0.42; 95% CI 0.15, 0.89). Another single center retrospective study [227] among 1178 hospitalized patients with COVID-19, had 362 patients with hypertension and 115 were on ACEI/ARBs. There was no difference between those with severe vs non-severe illness in use of ACEIs (9.2% vs 10.1%; P = .80), and ARBs (24.9% vs 21.2%; P = 0.40). There was also no difference between non-survivors and survivors in use of ACEIs (9.1% vs 9.8%; P = 0.85) and ARBs (19.5% vs 23.9%; P = 0.42).
Another study [228] among 1200 COVID-19 patients hospitalized in two hospitals in London, UK observed that chronic ACEI/ARB use was not associated with an increase in severity of COVID-19. Within their cohort of 1200 patients, 399 (33.3%) were on an ACEI/ARB and while unadjusted odds of critical care admission or death within 21 days were not significantly different between patients on ACEI/ARB vs not (OR 0.83; 95% CI 0.64, 1.07), adjustment for age, sex and co-morbidities presented an OR of 0.63 (95% CI 0.47, 0.84, p<0.01) for the composite outcomes in patients on ACEI/ARB. An observational study from Italy [229] evaluated multiple predictors of in-hospital mortality in 311 patients with hypertension and COVID-19. The patients in this study were significantly older, with a higher BMI, comorbidities, and severity of disease. In a multivariate Cox regression analysis chronic use of ACEI and ARBs (aHR, 0.97; 95% CI: 0.68, 1.39; P = .88) were not associated with an increase in in-hospital mortality. A population-based case-control study [216] from Lombardy, Italy compared 6272 COVID-19 patients with 30,759 controls matched on sex, age, and municipality of residence. In a logistic-regression multivariate analysis, use of ARBs or ACEI did not show an association with COVID-19 among cases (aOR, 0.95, 95% CI 0.86 to 1.05 for ARBs and 0.96, 95% CI, 0.87 to 1.07 for ACEI). It also did not show an association with severe or fatal disease (for ARBs, aOR 0.83; 95% CI 0.63, 1.10; for ACEI, aOR 0.91; 95% CI 0.69, 1.21). Reynolds et al [230] analyzed data available for patients tested for COVID-19, available in the electronic medical records for New York University Langone Health system. In the study, 12,594 patients were tested, 5,894 (46.8%) were positive and 1,002 of these patients (17.0%) had severe illness. They performed propensity score matching and a Bayesian analysis to assess the relationship between various classes of antihypertensives including ACEI and ARBs and the likelihood of a positive COVID-19 test and severe disease. The study did not show a positive association for ACEI and ARBs with having a positive test for SARS-CoV-2 or developing severe infection. A retrospective cohort study using data from Danish national administrative registries, had an unadjusted 30-day mortality of 18.1% in the group with ACEI/ARB use compared to the 7.3% in the nonuser group, but the association was not significant after adjustment for age, sex and medical history (aHR 0.83; 95% CI: 0.67, 1.03). In that study, ACEI/ARB use compared with other antihypertensive agents was not significantly associated with higher incidence of COVID-19 (a HR 1.05 95% CI 0.80–1.36) [231]. One retrospective cohort study done in severe COVID-19 patient's showed ACEI/ARB use, after adjusting for other variables, to be independently associated with elevated creatinine >10.1 mg/L (OR 3.22; 95% CI: 2.28, 4.54). Consistent ACEI/ARB use was independently associated with AKI stage >1 (ALT ratio 3.28; 95% CI: 2.17, 4.94) [232].
Data from these observational studies suggest that ACEI and ARBs do not increase the risk of acquiring COVID-19, developing severe disease or death. One study showed possible increase risk of renal dysfunction in severe COVID-19. There are limitations though inherent to retrospective observational studies, especially differences in unmeasured prognostic factors between the compared groups that might be responsible for the difference in outcomes and not treatment with ACEI or ARBs. Most professional scientific and medical societies have recommended that ACEI or ARBs be continued in people who have an indication for these medications [233-235].
Antibacterials and antifungals
Last reviewed and updated 9/4/2020
Patients with COVID-19 often present to hospitals with viral pneumonia with accompanying febrile illness and respiratory symptoms. Differential diagnoses may include bacterial pneumonia, for which antibiotics are prescribed. Concerns for bacterial superinfections also exist. Studies performed early in the COVID-19 pandemic reported high percentages of antibiotic use in China (58-95%) [1, 203, 236], Spain (74%) [237], and New York (65%) [238]. These studies are not granular and do not report if they describe co-infection at presentation or the development of superinfection, limiting the ability to ascertain the reasons for antibiotic use.
Data reporting co-infection in patients presenting with COVID-19 for care is sparse. Rawson and colleagues reviewed 18 studies of human coronavirus infections reporting co-infections, of which nine were COVID-19 [239]. These cumulatively reported a bacterial and fungal co-infection rate of 8% (62/806). The studies evaluated were heterogeneous. One brief report of 393 patients in New York reported a bacteremia rate of 5.6%, which varied significantly between patients receiving invasive mechanical ventilation (15/126 [11.9%]) and those who were not (4/222 [1.8%]) [240]. Another study looked at 88,201 blood cultures performed during March 2020 in New York, comparing order volume, positivity, and etiologies between patients with COVID-19 and others during the time period [241]. The study found a significantly lower rate of bacteremia in COVID-19 patients (3.8%) than either COVID-19 negative (8%) or untested (7.1%) (p<0.001). When commensal skin organisms were excluded, the positivity rate in COVID-19 patients was 1.6% [241]. A study in Texas reviewed the use of antibiotics and incidence of coinfections in 147 PCR-positive COVID-19 patients [242]. Eighty-seven (59%) patients received empiric antibiotics, though none of the 47 (32%) patients with respiratory cultures had positive results. 112 patients (76%) had blood cultures collected also, and while nine were positive, eight of those were considered contaminants [242].
The apparent discordance between bacterial and fungal co-infection in patients with COVID-19 at presentation and the use of antibacterial therapy has potential negative effects, namely in antimicrobial resistance. Publications report on patients with severe and critical COVID-19 patients treated with immunomodulatory therapies, including corticosteroids, IL-6 antagonists, IL-1 antagonists, and others [243]. In one preprint examining outcomes of in a cohort of 154 patients receiving invasive mechanically ventilation, mortality was reduced in patients treated with tocilizumab (IPTW-adjusted model, HR 0.55; 95% CI 0.33, 0.90); however, superinfections were more commonly reported (54% vs 26%, p<0.001), primarily due to ventilator-associated pneumonia [110]. Initiating and continuing empiric antibiotics at the time of admission may lead to superinfections that are antibiotic resistant [244].
Favipiravir
Last reviewed and updated 9/4/2020
Favipiravir is a purine analogue that inhibits the RNA dependent RNA polymerase of influenza and other RNA viruses [245]. The drug is approved in Japan for treatment of influenza. However, because of its teratogenicity risk, favipiravir should not be given during pregnancy and there are substantial concerns about its use in women in child-bearing potential.
In terms of its potential role in COVID-19, favipiravir has in vitro activity against SARS-CoV-2 [16]. However, it is uncertain whether adequate drug levels can be achieved in vivo to inhibit SARS-CoV-2. There have been small clinical trials with this drug in people with COVID-19. In a non-randomized, open-label study in China [246], oral favipiravir was associated with shorter time to viral clearance and greater improvement in chest imaging than lopinavir/ritonavir (in both groups, the oral antiviral was given with aerosolized alpha-interferon). However, because the study was small and not randomized, it was not possible to conclude that favipiravir is effective in treating COVID-19. A randomized, open-label trial compared favipiravir to umifenovir, an antiviral approved in Russia and China, in people with COVID-19 [247]. The clinical recovery rate at day seven was not significantly different between the two groups. There appeared to be an impact of favipiravir in the sub-group of people who did not have critical illness, but more data are needed. An exploratory clinical trial, also conducted in China, randomized 30 hospitalized adults with COVID-19 into a baloxavir marboxil, favipiravir or control group. There was no apparent effect of favipiravir (or baloxivir) on viral clearance [248]. There are ongoing clinical trials assessing favipiravir for treatment of COVID-19.
Immunomodulatory agents
Last reviewed and updated 9/4/2020
Some patients with COVID-19 develop a hyperinflammatory state that may incorporate elements of cytokine release syndrome seen in conditions such as secondary hemophagocytic lymphohistiocytosis (sHLH). The etiology is unclear, but patients who develop significantly elevated CRP, ferritin, and D-dimer levels with the syndrome have an increased risk of mortality, associated with respiratory failure, multiorgan dysfunction, and hypercoagulability. Numerous immunomodulatory agents are under investigation to address this immunologic complication.
IL-1 inhibitors: Anakinra is an FDA approved IL-1-beta inhibitor that is currently FDA-approved for rheumatoid arthritis and Neonatal-Onset Multisystem Inflammatory Disease. High- and low-dose anakinra was investigated in a recent retrospective cohort study in Italian patients with COVID-19, moderate to severe ARDS, and hyperinflammation. Patients receiving anakinra were compared to a historical control group with COVID-19 who fulfilled eligibility criteria for anakinra. The low-dose anakinra group was stopped early due to lack of effect. In the high-dose anakinra group, 3/29 (10%) patients died vs. 7/16 (44%) in the historical control group, however there was no difference in the rates of mechanical ventilation-free survival [249]. Anakinra is being investigated in numerous trials including this randomized placebo-controlled trial [250]. Canakinumab is another IL-1-beta antagonist with limited human data for COVID-19 that is being studied in a phase III clinical trial [251, 252].
Janus kinase inhibitors: Baricitinib, a Janus kinase inhibitor (anti-JAK) currently FDA-approved for the treatment of rheumatoid arthritis, is being investigated in multiple studies for COVID-19. The proposed benefits of baricitinib in the management of COVID-19 are two-fold as it has both anti-inflammatory and likely antiviral activity. Janus kinase mediates cytokine signaling which contributes to inflammation, which may reduce risk of the associated hyperinflammatory syndrome and ARDS. Baricitinib inhibits AAK1 and also binds GAK, both thought to play a role in receptor mediated endocytosis of many viruses including SARS-CoV-2 [154]. In an open-label non-randomized study from Italy, baricitinib with lopinavir/ritonavir (n=12) were compared to lopinavir/ritonavir (n=12) alone at one institution over two consecutive time periods. After two weeks in the baricitinib group, no patients required ICU transfer and 7/12 (58%) were discharged. In the lopinavir/ritonavir group, 4/12 (33%) required ICU transfer and only 1/12 patients were discharged by day 14. No serious adverse events or infections occurred in the baricitinib group [155]. In the ACTT-2 trial, baricitinib is being compared to remdesivir and numerous other RCTs are currently underway to better understand the role of baricitinib in the management of COVID-19 [253-257].
GM-CSF inhibitors: Monoclonal antibodies that bind to GM-CSF are under investigation for the treatment of hyperinflammation associated with COVID-19. GM-CSF inhibitors are postulated to disrupt the downstream signaling of pro-inflammatory cytokines. One agent, mavrilimumab was studied in a single center non-randomized cohort study in non-ventilated patients in Italy. Trial participants had SARS-CoV-2 infection with a PaO2: FiO2 ratio < 300 mm Hg, pulmonary infiltrates, and evidence of hyperinflammation (CRP > 100 mg/L or ferritin > 900 µg/L and any increase in LDH). Patients in the treatment group received a single dose of mavrilimumab 6 mg/kg (n=13). A similar cohort managed by the same medical team received no mavrilimumab due to lack of consent and lack of access to mavrilimumab (n=26). Mortality rates were 0/13 in the mavrilimumab group and 7/26 (27%) died in the control group. Median days to clinical improvement (defined as a reduction of two or more points on the seven-point ordinal scale) was 8 (IQR: 5-11) vs. 19 (IQR: 11- > 28), in the mavrilimumab vs. control groups, respectively. Mavrilimumab was well tolerated in all patients [258]. Randomized controlled trials are underway to investigate the role of GM-CSF inhibitors in the management of COVID-19 [259-261].
Complement inhibitors: ln mouse models of both SARS-CoV and MERS-CoV, complement activation has been shown to play a role in the pathogenesis of ARDS. Eculizumab, is a complement inhibitor that is already approved by the FDA for other conditions including myasthenia gravis and paroxysmal nocturnal hemoglobinuria, is currently being studied for the treatment of COVID-19 [262]. Ravulizumab, another complement inhibitor, is also being investigated in randomized trials for COVID-19 [254].
SARS-CoV-2 in children and treatment of multisystem inflammatory syndrome in children (MIS-C)
Last reviewed and updated 9/4/2020
Treatment
Compared with adults, children generally have milder illness from SARS-CoV-2 infection [263, 264]. However, severe illness does occur in children, even those with no predisposing factors [264, 265]. Among children admitted to the hospital for COVID-19, one-third are admitted to intensive care [264]. Despite this, clinical trials of therapeutic interventions for COVID-19 have almost exclusively focused on adult patients. For example, in the first of two recent studies of the antiviral remdesivir [266, 267], patients younger than 18 years were excluded [268], and the number of children between 12 and 18 years included in the analysis for the second paper was not reported [133]. These studies led to FDA EUA of remdesivir for both adults and children [269], with no published data available on either safety or efficacy in children under 12 years. A phase II/III open label study in this population has started (the “CARAVAN” trial [135]). Future studies of both therapeutics and vaccines will need to include children to assure their safety and efficacy in this population.
Multisystem inflammatory syndrome in children
Multisystem inflammatory syndrome in children (MIS-C) or Pediatric Multisystem Inflammatory Syndrome (PMIS) is a rare acute inflammatory syndrome with some similarities to Kawasaki disease that has recently been reported in children. Reports from Europe and the United States generally describe critically ill children with fever, rash, conjunctivitis, abdominal complaints, shock, and significant cardiac dysfunction [270-282]. Case definitions have been developed to better characterize these patients (Table 22) [283, 284].
Patients with Kawasaki disease also present with fever and symptoms including rash, conjunctivitis, peripheral extremity changes, lymphadenopathy, and oral mucosal changes such as red, cracked lips and “strawberry tongue.” However, while Kawasaki disease and MIS-C share some similarities, there are also key differences [285]. Both are hyperinflammatory syndromes, both have findings of medium vessel vasculitis and both can present with the signs/symptoms described for Kawasaki disease. MIS-C is more likely to affect older children (average age 8-11 years vs. younger than five years in Kawasaki disease), cause more severe disease (more patients presenting with shock), present frequently with gastrointestinal symptoms, includes some neurologic involvement, and more commonly causes cardiac myocarditis and ventricular dysfunction leading to hypotension or arrhythmias. In contrast, Kawasaki disease more commonly causes coronary artery dilatation. A small study of cytokine profiles in children distinguished MIS-C from severe COVID-19 based on a higher level of the combination of TNF-α and IL-10 in MIS-C patients [286].
Empiric treatment of MIS-C has generally involved immunomodulatory agents such as high-dose intravenous immunoglobulin (2 g/kg), corticosteroids, aspirin and rarely more targeted anti-inflammatory medications such as anakinra [270-273, 279, 280, 282]. Most of the children with MIS-C have had a history of prior SARS-CoV-2 infection several weeks earlier confirmed by viral detection of antibody testing or have had documented prior exposure to COVID-19, suggesting that this condition is a post-infectious immunologic phenomenon.
Future research should focus on how and why the immune system responds to SARS-CoV-2 causing a spectrum of illness in children, identifying genetic or environmental risk factors for MIS-C, and discovering optimum treatment for children with MIS-C. Multidisciplinary, collaborative approaches to data registries and clinical trials that promote evidence-based care for these children are needed.
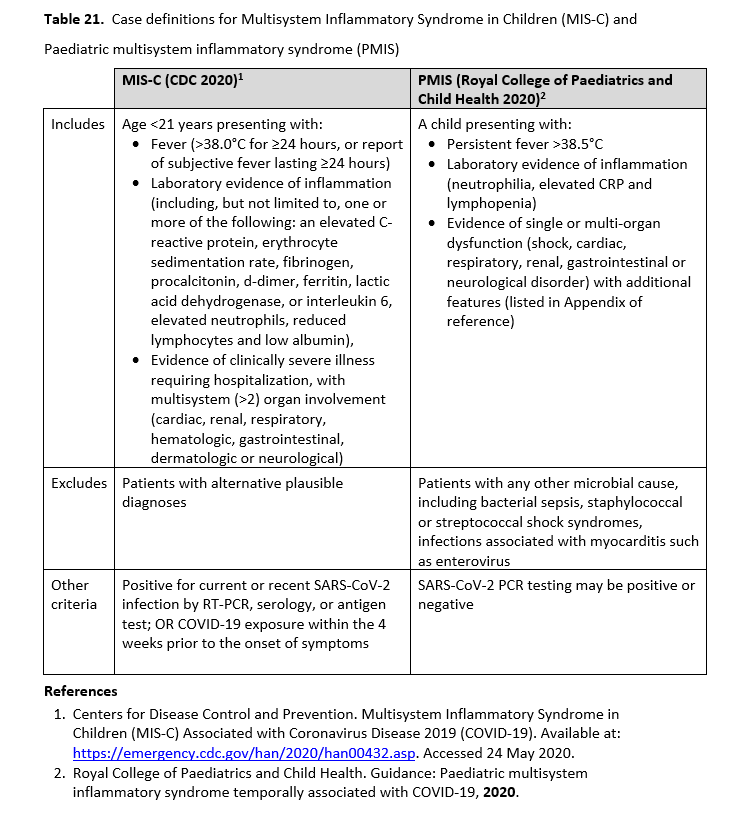
References
- Centers for Disease Control and Prevention. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). Available at: https://emergency.cdc.gov/han/2020/han00432.asp. Accessed 24 May 2020.
- Royal College of Paediatrics and Child Health. Guidance: Paediatric multisystem inflammatory syndrome temporally associated with COVID-19, 2020.
Discussion
During epidemics like the current COVID-19 pandemic, when there are no clinically proven treatments, the tendency is to use drugs based on in vitro antiviral activity, or on anti-inflammatory effects or based on limited observational studies. It is commendable that observational studies are done during an epidemic, but often they do not have concurrent controls, have a significant risk of bias, and use surrogate outcomes like viral clearance rather than patient-important outcomes. Medications that were thought to be effective based on in vitro studies and observational studies for other diseases were later proven to be ineffective in clinical trials [287].
Due to the understandable urgency in producing, synthesizing and disseminating data during the current pandemic, there has been a noticeable increase in fast track publication of studies. In addition to well-established concerns that may decrease our certainty in the available evidence, there may be additional issues that will ultimately influence the trustworthiness of that evidence, including: 1) Circumvention of usual research steps (delay of IRB approval [288], inclusion of same patients in several studies); 2) Limited peer-review process (the usual due diligence from editors and reviewers is side-stepped, potentially leading to unnoticed errors in data and calculations, incomplete reporting of methods and results, as well as underestimation of study limitations); 3) Increased potential for publication bias (in the interest of showing promising data and in the race to achieve recognition, there may be added inclination to publish positive results and disregard negative ones). The extent and impact of these considerations remain currently uncertain but were acknowledged in the development of this guideline.
Despite these limitations, the recommendations in this guideline are based on evidence from the best available clinical studies with patient-important endpoints. The panel determined that when an explicit trade-off between the highly uncertain benefits (e.g., the panel was unable to confirm that HCQ increases viral cure or reduces mortality) and the known putative harms (QT prolongation and drug-drug interactions) were considered, a net positive benefit was not reached and could possibly be negative (risk of excess harm). The safety of drugs used for the treatment of COVID-19, especially in patients with cardiovascular disease, immunosuppressive conditions, or those who are critically ill with multi-organ failure has also not been studied. Drugs like AZ and HCQ can cause QT prolongation and potentially life-threatening arrhythmias. Steroids and IL-6 inhibitors can be immunosuppressive and potentially increase risk of secondary infections. Steroids may produce long term side effect such as osteonecrosis [289]. In instances where the panel could not make a determination whether the benefits outweigh harms, it is be ethical and prudent to enroll patients with COVID-19 in clinical trials, rather than use clinically unproven therapies [290]. There are multiple ongoing trials, some with adaptive designs, which potentially can quickly answer pressing questions on efficacy and safety of drugs in the treatment of patients with COVID-19.
We acknowledge that enrolling patients in RCTs might not be feasible for many frontline providers due to limited access and infrastructure. Should lack of access to clinical trials exist, we encourage setting up local or collaborative registries to systematically evaluate the efficacy and safety of drugs to contribute to the knowledge base. Without such evaluations we often attribute success to drugs and failure to disease (COVID-19) [287]. During such a pandemic, barriers to conducting studies and enrolling patients in trials for already overburdened front line providers should be minimized while ensuring the rights and safety of patients [291].
For clinical trials and observational studies, it is critical to determine a priori standardized and practical definitions of patient populations, clinical syndromes, disease severity and outcomes. Observational and non-experimental studies can sometimes answer questions not addressed by trials, but there is still a need for standardized definitions. For clinical syndromes clearly distinguishing between asymptomatic carrier state, upper respiratory tract infection and lower respiratory tract infection is important. Illness severity should be reasonably defined using readily available clinical criteria of end organ failure, like the degree of respiratory failure using SpO2 (percentage of oxyhemoglobin saturation) or PaO2:FiO2 ratios (partial pressure of oxygen in arterial blood: fractional percentage of inspired oxygen) for lower respiratory tract infection, as opposed to location-based severity determinations such as ICU admission, which can lead to bias based on resource limitations (i.e., bed availability) or regional/institutional practice patterns [292]. For outcomes of prophylaxis trials, the primary endpoint should be prevention of infection and for therapeutic trials patient centered outcomes like reduction of mortality (both short term and long term) [293]. Trials should also study treatments in high risk populations or special populations like immunosuppressed patients, people with HIV, patients with cardiovascular comorbidities and pregnant women. The panel expressed the overarching goal that patients be recruited into ongoing trials, which would provide much needed evidence on the efficacy and safety of various therapies for COVID-19.
This is a living guideline that will be frequently updated as new data emerges. Updates and changes to the guideline will be posted to the IDSA website.
Notes
Acknowledgement
The expert panel thanks the Infectious Diseases Society of America for supporting guideline development, and specifically Cindy Sears, Dana Wollins, Genet Demisashi, and Rebecca Goldwater for their continued support throughout the guideline process. The panel would also like to acknowledge Haya Waseem, Kapeena Sivakumaran, and Nicholas J. Newman for supporting the evidence base for this guideline.
Financial Support
This project was funded in part by a cooperative agreement with the Centers for Disease Control and Prevention (CDC) (grant number 6 NU50CK000477-04-01). The CDC is an agency within the Department of Health and Human Services (HHS). The contents of this guideline do not necessarily represent the policy of CDC or HHS and should not be considered an endorsement by the Federal Government.
COI Summary
The following list is a reflection of what has been reported to the IDSA. To provide thorough transparency, the IDSA requires full disclosure of all relationships, regardless of relevancy to the guideline topic. Evaluation of such relationships as potential conflicts of interest is determined by a review process which includes assessment by the Board of Directors liaison to the Standards and Practice Guideline Committee and, if necessary, the Conflicts of Interest (COI) and Ethics Committee. The assessment of disclosed relationships for possible COI is based on the relative weight of the financial relationship (i.e., monetary amount) and the relevance of the relationship (i.e., the degree to which an association might reasonably be interpreted by an independent observer as related to the topic or recommendation of consideration). The reader of these guidelines should be mindful of this when the list of disclosures is reviewed. L.B. receives research funding from the National Institutes of Health/National Institute of Allergy and Infectious Diseases, Bill and Melinda Gates Foundation, and Wellcome Trust, and serves as chair of the Antimicrobial Drug Advisory Committee of the Food and Drug Administration. V.C. receives research funding from the Health and Medical Research Fund. K. E. serves as a scientific advisor for Merck, Bionet, IBM, Sanofi, X4 Pharmaceuticals, Inc., Seqirus, Inc., Moderna, Inc. and Pfizer, and receives research funding from the Centers for Disease Control and Prevention and the National Institutes of Health. R. G. has served on a scientific advisory board for Gilead Sciences, Inc., serves on a scientific advisory board for Merck, and receives research funding from the NIH. J.G. serves in an advisory role for Qpex and Shionogi; receives research funding from Merk; previously served in an advisory role for Acceletrate, Achaogen, Astellas, Melinta, Nabriva, Paratek, scPharmaceutic, Spero and Tetraphase; and previously served on the speakers bureau for Astellas, Melinta, Merck and Shiongi. M.H.M receives research funding from the Agency for Healthcare Research and Quality, the Endocrine Society, the Society for Vascular Surgery and The American Society of Hematology and is a Board member for the Evidence Foundation. W.J.M. serves in an advisory role for Seqirus, Inc. and receives research funding from Ansun Biopharma, Astellas Pharma, AstraZeneca, Abbott Laboratories, Enanta Pharmaceuticals, Gilead Sciences, Janssen Pharmaceuticals, Karius, Merck, Melinta Therapeutics, Nabriva Therapeutics, Roche and Tetraphase Pharmaceuticals. S.S. serves as an advisory board member for Amplyx Pharmaceuticals, Inc.; as an advisor/consultant to ReViral Ltd.; receives research funding from Ansun BioPharma, F2G, Shire (now Takeda), University of Nebraska, Cidara Therapeutics; and has served as an advisor for Janssen Pharmaceutica and Acidophil. A.H.S. receives research funding from the U.S. Department of Veterans Affairs. Y.F.Y. receives honoraria for evidence reviews and teaching from the Evidence Foundation, honoraria for evidence reviews for the American Gastroenterological Association, and serves as a Director for the Evidence Foundation and for the U.S. GRADE Network. All other authors: no disclosures reported. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. All other authors: no disclosures reported.
IDSA Disclaimer
It is important to realize that guidelines cannot always account for individual variation among patients. They are assessments of current scientific and clinical information provided as an educational service; are not continually updated and may not reflect the most recent evidence (new evidence may emerge between the time information is developed and when it is published or read); should not be considered inclusive of all proper treatments methods of care, or as a statement of the standard of care; do not mandate any particular course of medical care; and are not intended to supplant physician judgment with respect to particular patients or special clinical situations. Whether and the extent to which to follow guidelines is voluntary, with the ultimate determination regarding their application to be made by the physician in the light of each patient’s individual circumstances. While IDSA makes every effort to present accurate, complete, and reliable information, these guidelines are presented “as is” without any warranty, either express or implied. IDSA (and its officers, directors, members, employees, and agents) assume no responsibility for any loss, damage, or claim with respect to any liabilities, including direct, special, indirect, or consequential damages, incurred in connection with these guidelines or reliance on the information presented.
The guidelines represent the proprietary and copyrighted property of IDSA. Copyright 2020 Infectious Diseases Society of America. All rights reserved. No part of these guidelines may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of IDSA. Permission is granted to physicians and health care providers solely to copy and use the guidelines in their professional practices and clinical decision-making. No license or permission is granted to any person or entity, and prior written authorization by IDSA is required, to sell, distribute, or modify the guidelines, or to make derivative works of or incorporate the guidelines into any product, including but not limited to clinical decision support software or any other software product. Except for the permission granted above, any person or entity desiring to use the guidelines in any way must contact IDSA for approval in accordance with the terms and conditions of third-party use, in particular any use of the guidelines in any software product.
References
-
- Guan WJ, Ni ZY, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 2020.
- World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report - 75. Geneva: World Health Organization, 2020 4 April.
- Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020.
- Morgan RL, Florez I, Falavigna M, et al. Development of rapid guidelines: 3. GIN-McMaster Guideline Development Checklist extension for rapid recommendations. Health Res Policy Syst 2018; 16(1): 63.
- Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol 2011; 64(4): 395-400.
- U.S. Food and Drug Administration. What is a Serious Adverse Event? Available at: https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event. Accessed 19 June 2020.
- National Institute for Health and Care Excellence. Scoping. Interim process and methods for developing rapid guidelines on COVID-19 (PMG35). London: National Institute for Health and Care Excellence, 2020.
- Wallace BC, Dahabreh IJ, Trikalinos TA, Lau J, Trow P, Schmid CH. Closing the gap between methodologists and end-users: R as a computational back-end. J Stat Softw 2012; 49(5): 1-15.
- Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. 2 ed. Chichester (UK): John Wiley & Sons, 2019.
- Sterne JA, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016; 355: i4919.
- Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011; 64(4): 383-94.
- GRADEpro GDT. GRADEpro Guideline Development Tool [Software]. McMaster University, 2015 (developed by Evidence Prime, Inc.). Available at: https://gradepro.org/.
- Ben-Zvi I, Kivity S, Langevitz P, Shoenfeld Y. Hydroxychloroquine: from malaria to autoimmunity. Clin Rev Allergy Immunol 2012; 42(2): 145-53.
- Keyaerts E, Vijgen L, Maes P, Neyts J, Van Ranst M. In vitro inhibition of severe acute respiratory syndrome coronavirus by chloroquine. Biochem Biophys Res Commun 2004; 323(1): 264-8.
- Dyall J, Coleman CM, Hart BJ, et al. Repurposing of clinically developed drugs for treatment of Middle East respiratory syndrome coronavirus infection. Antimicrob Agents Chemother 2014; 58(8): 4885-93.
- Wang M, Cao R, Zhang L, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res 2020; 30(3): 269-71.
- Yao X, Ye F, Zhang M, et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin Infect Dis 2020.
- Vincent MJ, Bergeron E, Benjannet S, et al. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol J 2005; 2: 69.
- Gautret P, Lagier JC, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents 2020; 56(1): 105949.
- Li C, Zu S, Deng YQ, et al. Azithromycin Protects against Zika virus Infection by Upregulating virus-induced Type I and III Interferon Responses. Antimicrob Agents Chemother 2019.
- Kouznetsova J, Sun W, Martinez-Romero C, et al. Identification of 53 compounds that block Ebola virus-like particle entry via a repurposing screen of approved drugs. Emerg Microbes Infect 2014; 3(12): e84.
- Gielen V, Johnston SL, Edwards MR. Azithromycin induces anti-viral responses in bronchial epithelial cells. Eur Respir J 2010; 36(3): 646-54.
- Tyteca D, Van Der Smissen P, Mettlen M, et al. Azithromycin, a lysosomotropic antibiotic, has distinct effects on fluid-phase and receptor-mediated endocytosis, but does not impair phagocytosis in J774 macrophages. Exp Cell Res 2002; 281(1): 86-100.
- Menzel M, Akbarshahi H, Bjermer L, Uller L. Azithromycin induces anti-viral effects in cultured bronchial epithelial cells from COPD patients. Sci Rep 2016; 6: 28698.
- Takizawa H, Desaki M, Ohtoshi T, et al. Erythromycin suppresses interleukin 6 expression by human bronchial epithelial cells: a potential mechanism of its anti-inflammatory action. Biochem Biophys Res Commun 1995; 210(3): 781-6.
- Schultz MJ. Macrolide activities beyond their antimicrobial effects: macrolides in diffuse panbronchiolitis and cystic fibrosis. J Antimicrob Chemother 2004; 54(1): 21-8.
- Arshad S, Kilgore P, Chaudhry ZS, et al. Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalized with COVID-19. Int J Infect Dis 2020; 97: 396-403.
- Cavalcanti AB, Zampieri FG, Rosa RG, et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19. N Engl J Med 2020; 383: 2041-52.
- Horby P, Mafham M, Linsell L, et al. Effect of Hydroxychloroquine in Hospitalized Patients with COVID-19: Preliminary results from a multi-centre, randomized, controlled trial. medRxiv 2020.
- Chen J, Liu D, Liu L, et al. A pilot study of hydroxychloroquine in treatment of patients with moderate COVID-19. Journal of Zhejiang University (Medical Sciences) 2020; 49(2): 215-9.
- Chen Z, Hu J, Zhang Z, et al. Efficacy of hydroxychloroquine in patients with COVID-19: results of a randomized clinical trial. medRxiv 2020: Available at: https://doi.org/10.1101/2020.03.22.20040758 [Preprint 10 April 2020].
- WHO Solidarity Trial Consortium, Pan H, Peto R, et al. Repurposed Antiviral Drugs for Covid-19 — Interim WHO Solidarity Trial Results. N Engl J Med 2021; 384: 497-511.
- Self WH, Semler MW, Leither LM, et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients With COVID-19: A Randomized Clinical Trial. JAMA 2020; 324(21): 2165-76.
- Ulrich RJ, Troxel AB, Carmody E, et al. Treating COVID-19 With Hydroxychloroquine (TEACH): A Multicenter, Double-Blind Randomized Controlled Trial in Hospitalized Patients. Open Forum Infect Dis 2020; 7(10): ofaa446.
- Tang W, Cao Z, Han M, et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial. BMJ 2020; 369: m1849.
- Geleris J, Sun Y, Platt J, et al. Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19. N Engl J Med 2020.
- Magagnoli J, Narendran S, Pereira F, et al. Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19. Med 2020; 1(1): 114-27.e3.
- Mahevas M, Tran V-T, Roumier M, et al. No evidence of clinical efficacy of hydroxychloroquine in patients hospitalized for COVID-19 infection with oxygen requirement: results of a study using routinely collected data to emulate a target trial. medRxiv 2020: Available at: https://doi.org/10.1101/2020.04.10.20060699 [Preprint 14 April 2020].
- Rosenberg ES, Dufort EM, Udo T, et al. Association of treatment with hydroxychloroquine or azithromycin with in-hospital mortality in patients with COVID-19 in New York state. JAMA 2020; 323(24): 2493-502.
- Yu B, Li C, Chen P, et al. Low dose of hydroxychloroquine reduces fatality of critically ill patients with COVID-19. Sci China Life Sci 2020.
- Ip A, Berry DA, Hansen E, et al. Hydroxychloroquine and Tocilizumab Therapy in COVID-19 Patients-An Observational Study. PloS One 2020; 15(8): e0237693.
- Cipriani A, Zorzi A, Ceccato D, et al. Arrhythmic profile and 24-hour QT interval variability in COVID-19 patients treated with hydroxychloroquine and azithromycin. Int J Cardiol 2020.
- Molina JM, Delaugerre C, Goff J, et al. No Evidence of Rapid Antiviral Clearance or Clinical Benefit with the Combination of Hydroxychloroquine and Azithromycin in Patients with Severe COVID-19 Infection. Médecine et Maladies Infectieuses 2020; 50(4): 384.
- Gautret P, Lagier JC, Parola P, et al. Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: A pilot observational study. Travel Med Infect Dis 2020; 34: 101663.
- Chorin E, Dai M, Shulman E, et al. The QT Interval in Patients with SARS-CoV-2 Infection Treated with Hydroxychloroquine/Azithromycin. medRxiv 2020: Available at: https://doi.org/10.1101/2020.04.02.20047050 [Preprint 3 April 2020].
- Wang C, Fortin PR, Li Y, Panaritis T, Gans M, Esdaile JM. Discontinuation of antimalarial drugs in systemic lupus erythematosus. J Rheumatol 1999; 26(4): 808-15.
- Youngster I, Arcavi L, Schechmaster R, et al. Medications and glucose-6-phosphate dehydrogenase deficiency: an evidence-based review. Drug Saf 2010; 33(9): 713-26.
- Mohammad S, Clowse MEB, Eudy AM, Criscione-Schreiber LG. Examination of Hydroxychloroquine Use and Hemolytic Anemia in G6PDH-Deficient Patients. Arthritis Care Res (Hoboken) 2018; 70(3): 481-5.
- Beauverd Y, Adam Y, Assouline B, Samii K. COVID-19 infection and treatment with hydroxychloroquine cause severe haemolysis crisis in a patient with glucose-6-phosphate dehydrogenase deficiency. Eur J Haematol 2020.
- Kuipers MT, van Zwieten R, Heijmans J, et al. G6PD deficiency-associated hemolysis and methemoglobinemia in a COVID-19 patient treated with chloroquine. Am J Hematol 2020.
- Maillart E, Leemans S, Van Noten H, et al. A case report of serious haemolysis in a glucose-6-phosphate dehydrogenase-deficient COVID-19 patient receiving hydroxychloroquine. Infect Dis (Lond) 2020: 1-3.
- Rainsford KD, Parke AL, Clifford-Rashotte M, Kean WF. Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases. Inflammopharmacology 2015; 23(5): 231-69.
- Morgan ND, Patel SV, Dvorkina O. Suspected hydroxychloroquine-associated QT-interval prolongation in a patient with systemic lupus erythematosus. J Clin Rheumatol 2013; 19(5): 286-8.
- Chen CY, Wang FL, Lin CC. Chronic hydroxychloroquine use associated with QT prolongation and refractory ventricular arrhythmia. Clin Toxicol (Phila) 2006; 44(2): 173-5.
- Yelve K, Phatak S, Patil MA, Pazare AR. Syncope in a patient being treated for hepatic and intestinal amoebiasis. BMJ Case Rep 2012; 2012.
- Stas P, Faes D, Noyens P. Conduction disorder and QT prolongation secondary to long-term treatment with chloroquine. Int J Cardiol 2008; 127(2): e80-2.
- Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM. Azithromycin and the risk of cardiovascular death. N Engl J Med 2012; 366(20): 1881-90.
- von Rosensteil NA, Adam D. Macrolide antibacterials. Drug interactions of clinical significance. Drug Saf 1995; 13(2): 105-22.
- Chen F, Chan KH, Jiang Y, et al. In vitro susceptibility of 10 clinical isolates of SARS coronavirus to selected antiviral compounds. J Clin Virol 2004; 31(1): 69-75.
- Wu CY, Jan JT, Ma SH, et al. Small molecules targeting severe acute respiratory syndrome human coronavirus. Proc Natl Acad Sci U S A 2004; 101(27): 10012-7.
- Chan JF, Yao Y, Yeung ML, et al. Treatment With Lopinavir/Ritonavir or Interferon-beta1b Improves Outcome of MERS-CoV Infection in a Nonhuman Primate Model of Common Marmoset. J Infect Dis 2015; 212(12): 1904-13.
- Chu CM, Cheng VC, Hung IF, et al. Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax 2004; 59(3): 252-6.
- Spanakis N, Tsiodras S, Haagmans BL, et al. Virological and serological analysis of a recent Middle East respiratory syndrome coronavirus infection case on a triple combination antiviral regimen. Int J Antimicrob Agents 2014; 44(6): 528-32.
- Kim UJ, Won EJ, Kee SJ, Jung SI, Jang HC. Combination therapy with lopinavir/ritonavir, ribavirin and interferon-alpha for Middle East respiratory syndrome. Antivir Ther 2016; 21(5): 455-9.
- Hung IF, Lung KC, Tso EY, et al. Triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, phase 2 trial. Lancet 2020; 395(10238): 1695-704.
- Cao B, Wang Y, Wen D, et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N Engl J Med 2020.
- RECOVERY Collaborative Group, Horby PW, Mafham M, et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. The Lancet 2020; 396(10259): 1345-52.
- World Health Organization. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected. Available at: https://apps.who.int/iris/bitstream/handle/10665/331446/WHO-2019-nCoV-clinical-2020.4-eng.pdf. Accessed 24 June 2020.
- Arabi YM, Mandourah Y, Al-Hameed F, et al. Corticosteroid Therapy for Critically Ill Patients with Middle East Respiratory Syndrome. Am J Respir Crit Care Med 2018; 197(6): 757-67.
- Lee N, Allen Chan KC, Hui DS, et al. Effects of early corticosteroid treatment on plasma SARS-associated Coronavirus RNA concentrations in adult patients. J Clin Virol 2004; 31(4): 304-9.
- Xiao JZ, Ma L, Gao J, et al. [Glucocorticoid-induced diabetes in severe acute respiratory syndrome: the impact of high dosage and duration of methylprednisolone therapy]. Zhonghua Nei Ke Za Zhi 2004; 43(3): 179-82.
- Laurent A, Bonnet M, Capellier G, Aslanian P, Hebert P. Emotional Impact of End-of-Life Decisions on Professional Relationships in the ICU: An Obstacle to Collegiality? Crit Care Med 2017; 45(12): 2023-30.
- Villar J, Ferrando C, Martinez D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med 2020; 8(3): 267-76.
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group, Sterne JAC, Murthy S, et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020.
- RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med 2021; 384: 693-704.
- Tomazini BM, Maia IS, Cavalcanti AB, et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020.
- Dequin PF, Heming N, Meziani F, et al. Effect of Hydrocortisone on 21-Day Mortality or Respiratory Support Among Critically Ill Patients With COVID-19: A Randomized Clinical Trial. JAMA 2020.
- Writing Committee for the REMAP-CAP Investigators, Angus DC, Derde L, et al. Effect of Hydrocortisone on Mortality and Organ Support in Patients With Severe COVID-19: The REMAP-CAP COVID-19 Corticosteroid Domain Randomized Clinical Trial. JAMA 2020.
- Petersen MW, Meyhoff TS, Helleberg M, et al. Low-dose hydrocortisone in patients with COVID-19 and severe hypoxia (COVID STEROID) trial-Protocol and statistical analysis plan. Acta Anaesthesiol Scand 2020.
- Jeronimo CMP, Farias MEL, Val FFA, et al. Methylprednisolone as Adjunctive Therapy for Patients Hospitalized With COVID-19 (Metcovid): A Randomised, Double-Blind, Phase IIb, Placebo-Controlled Trial. Clin Infect Dis 2020.
- Corral L, Bahamonde A, Arnaiz delas Revillas F, et al. GLUCOCOVID: A controlled trial of methylprednisolone in adults hospitalized with COVID-19 pneumonia. medRxiv 2020: 2020.06.17.20133579.
- Salton F, Confalonieri P, Santus P, et al. Prolonged low-dose methylprednisolone in patients with severe COVID-19 pneumonia. medRxiv 2020: 2020.06.17.20134031.
- Wang Y, Jiang W, He Q, et al. Early, low-dose and short-term application of corticosteroid treatment in patients with severe COVID-19 pneumonia: single-center experience from Wuhan, China. medRxiv 2020: 2020.03.06.20032342.
- Wu C, Chen X, Cai Y, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med 2020.
- Fernandez-Cruz A, Ruiz-Antoran B, Munoz-Gomez A, et al. Impact of glucocorticoid treatment in SARS-CoV-2 infection mortality: a retrospective controlled cohort study. medRxiv 2020: 2020.05.22.20110544.
- Lu X, Chen T, Wang Y, et al. Adjuvant corticosteroid therapy for critically ill patients with COVID-19. medRxiv 2020: 2020.04.07.20056390.
- Yuan M, Xu X, Xia D, et al. Effects of Corticosteroid Treatment for Non-Severe COVID-19 Pneumonia: A Propensity Score-Based Analysis. Shock 2020.
- Henzen C, Suter A, Lerch E, Urbinelli R, Schorno XH, Briner VA. Suppression and recovery of adrenal response after short-term, high-dose glucocorticoid treatment. Lancet 2000; 355(9203): 542-5.
- Siemieniuk RA, Meade MO, Alonso-Coello P, et al. Corticosteroid Therapy for Patients Hospitalized With Community-Acquired Pneumonia: A Systematic Review and Meta-analysis. Ann Intern Med 2015; 163(7): 519-28.
- Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest 2020; 130(5): 2620-9.
- Kalikshtein DB, Levantovskaia OM, Vyshenepol'skii I, Ol'shanskii A. [Coagulation and anticoagulation systems of the blood in allergic diseases]. Sov Med 1988; (9): 104-6.
- Regeneron Pharmaceuticals, Inc. Evaluation of the Efficacy and Safety of Sarilumab in Hospitalized Patients With COVID-19. Available at: https://clinicaltrials.gov/ct2/show/NCT04315298.
- Assistance Publique - Hôpitaux de Paris. Cohort Multiple Randomized Controlled Trials Open-label of Immune Modulatory Drugs and Other Treatments in COVID-19 Patients - Sarilumab Trial - CORIMUNO-19 - SARI (CORIMUNO-SARI). Available at: https://clinicaltrials.gov/ct2/show/NCT04324073.
- Branch-Elliman W. Sarilumab for Patients With Moderate COVID-19 Disease. Available at: https://clinicaltrials.gov/ct2/show/NCT04359901.
- Della-Torre E, Campochiaro C, Cavalli G, et al. Interleukin-6 blockade with sarilumab in severe COVID-19 pneumonia with systemic hyperinflammation: an open-label cohort study. Ann Rheum Dis 2020; 79(10): 1277-85.
- Gremese E, Cingolani A, Bosello SL, et al. Sarilumab use in severe SARS-CoV-2 pneumonia. EClinicalMedicine 2020; 27: 100553.
- Gordon AC, Mouncey PR, Al-Beidh F, et al. Interleukin-6 Receptor Antagonists in Critically Ill Patients with Covid-19 – Preliminary report. medRxiv 2021: Available at: https://www.medrxiv.org/content/10.1101/2021.01.07.21249390v2.full [Preprint 9 January 2021].
- Hermine O, Mariette X, Tharaux PL, et al. Effect of Tocilizumab vs Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial. JAMA Intern Med 2020; 181(1): 32-40.
- Horby PW, Pessoa-Amorim G, Peto L, et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): preliminary results of a randomised, controlled, open-label, platform trial. medRxiv 2021: Available at: https://doi.org/10.1101/2021.02.11.21249258 [Preprint 11 February 2021].
- Rosas I, Bräu N, Waters M, et al. Tocilizumab in hospitalized patients with COVID-19 pneumonia. MedRxiv 2020: Available at: https://doi.org/10.1101/2020.08.27.20183442 [Preprint 12 September 2020].
- Salama C, Han J, Yau L, et al. Tocilizumab in Patients Hospitalized with Covid-19 Pneumonia. N Engl J Med 2021; 384(1): 20-30.
- Salvarani C, Dolci G, Massari M, et al. Effect of Tocilizumab vs Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern Med 2020; 181(1): 24-31.
- Stone JH, Frigault MJ, Serling-Boyd NJ, et al. Efficacy of Tocilizumab in Patients Hospitalized with Covid-19. N Engl J Med 2020; 383: 2333-44.
- Veiga VC, Prats J, Farias DLC, et al. Effect of tocilizumab on clinical outcomes at 15 days in patients with severe or critical coronavirus disease 2019: randomised controlled trial. BMJ 2021; 372: n84.
- Rojo M, Cano-Valderrama O, Picazo S, et al. Gastrointestinal Perforation After Treatment With Tocilizumab : An Unexpected Consequence of COVID-19 Pandemic. Am Surg 2020; 86(6): 565-6.
- Gonzalvez Guardiola P, Diez Ares JA, Peris Tomas N, Sebastian Tomas JC, Navarro Martinez S. Intestinal perforation in patient with COVID-19 infection treated with tocilizumab and corticosteroids. Report of a clinical case. Cir Esp 2020.
- Ranchal P, Yates E, Gupta R, Aronow WS. Tocilizumab-Associated Bowel Perforation in SARS-CoV-2 Infection. Am J Ther 2020.
- Bruce-Hickman D, Sajeed SM, Pang YH, Seow CS, Chen W, Gulati Kansal M. Bowel ulceration following tocilizumab administration in a COVID-19 patient. BMJ Open Gastroenterol 2020; 7(1).
- Guaraldi G, Meschiari M, Cozzi-Lepri A, et al. Tocilizumab in patients with severe COVID-19: a retrospective cohort study. Lancet Rheumatol 2020; 2(8): e474-e84.
- Somers EC, Eschenauer GA, Troost JP, et al. Tocilizumab for treatment of mechanically ventilated patients with COVID-19. Clin Infect Dis 2020.
- Li L, Zhang W, Hu Y, et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients With Severe and Life-threatening COVID-19: A Randomized Clinical Trial. JAMA 2020; 324(5): 460-70.
- Gharbharan A, Jordans CC, GeurtsvanKessel C, et al. Convalescent Plasma for COVID-19. A randomized clinical trial. medRxiv 2020: Available at: https://doi.org/10.1101/2020.07.01.20139857 [Preprint 3 July 2020].
- AlQahtani M, Abdulrahman A, AlMadani A, et al. Randomized controlled trial of convalescent plasma therapy against standard therapy in patients with severe COVID-19 disease. medRxiv 2020: Available at: https://doi.org/10.1101/2020.11.02.20224303 [Preprint 4 November 2020].
- Avendaño-Solà C, Ramos-Martinez A, Muñez-Rubio E, et al. Convalescent plasma for COVID-19: a multicenter, randomized clinical trial. medRxiv 2020: Available at: https://doi.org/10.1101/2020.08.26.20182444 [Preprint 29 September 2020].
- Libster R, Marc GP, Wappner D, et al. Prevention of severe COVID-19 in the elderly by early high-titer plasma. medRxiv 2020: Available at: https://doi.org/10.1101/2020.11.20.20234013 [Preprint 21 November 2020].
- Joyner MJ, Senefeld JW, Klassen SA, et al. Effect of convalescent plasma on mortality among hospitalized patients with COVID-19: initial three-month experience. medRxiv 2020: Available at: https://doi.org/10.1101/2020.08.12.20169359 [Preprint 12 August 2020].
- Ray Y, Paul SR, Bandopadhyay P, et al. Clinical and immunological benefits of convalescent plasma therapy in severe COVID-19: insights from a single center open label randomised control trial. medRxiv 2020: Available at: https://doi.org/10.1101/2020.11.25.20237883 [Preprint 29 November 2020].
- Simonovich VA, Burgos Pratx LD, Scibona P, et al. A Randomized Trial of Convalescent Plasma in Covid-19 Severe Pneumonia. N Engl J Med 2021; 384(7): 619-29.
- Agarwal A, Mukherjee A, Kumar G, et al. Convalescent plasma in the management of moderate covid-19 in adults in India: open label phase II multicentre randomised controlled trial (PLACID Trial). BMJ 2020; 371: m4232.
- O’Donnell MR, Grinsztejn B, Cummings MJ, et al. A randomized, double-blind, controlled trial of convalescent plasma in adults with severe COVID-19. medRxiv 2021: Available at: https://doi.org/10.1101/2021.03.12.21253373 [Preprint 13 March 2021].
- U.S. Food and Drug Administration. Recommendations for Investigational COVID-19 Convalescent Plasma. Available at: https://www.fda.gov/vaccines-blood-biologics/investigational-new-drug-ind-or-device-exemption-ide-process-cber/recommendations-investigational-covid-19-convalescent-plasma. Accessed 28 August 2020.
- U.S. Food and Drug Administration. FDA In Brief: FDA Updates Emergency Use Authorization for COVID-19 Convalescent Plasma to Reflect New Data. Available at: https://www.fda.gov/news-events/fda-brief/fda-brief-fda-updates-emergency-use-authorization-covid-19-convalescent-plasma-reflect-new-data. Accessed 30 March 2021.
- Horby PW, Estcourt L, Peto L, et al. Convalescent plasma in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. medRxiv 2021: Available at: https://doi.org/10.1101/2021.03.09.21252736 [Preprint 10 March 2021].
- Balcells ME, Rojas L, Le Corre N, et al. Early versus deferred anti-SARS-CoV-2 convalescent plasma in patients admitted for COVID-19: A randomized phase II clinical trial. PLoS Med 2021; 18(3): e1003415.
- Joyner MJ, Bruno KA, Klassen SA, et al. Safety Update: COVID-19 Convalescent Plasma in 20,000 Hospitalized Patients. Mayo Clin Proc 2020; 95(9): 1888-97.
- Lo MK, Jordan R, Arvey A, et al. GS-5734 and its parent nucleoside analog inhibit Filo-, Pneumo-, and Paramyxoviruses. Sci Rep 2017; 7: 43395.
- Sheahan TP, Sims AC, Graham RL, et al. Broad-spectrum antiviral GS-5734 inhibits both epidemic and zoonotic coronaviruses. Sci Transl Med 2017; 9(396).
- Warren TK, Jordan R, Lo MK, et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 2016; 531(7594): 381-5.
- Williamson BN, Feldmann F, Schwarz B, et al. Clinical benefit of remdesivir in rhesus macaques infected with SARS-CoV-2. Nature 2020.
- Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med 2020; 383(19): 1813-26.
- Spinner CD, Gottlieb RL, Criner GJ, et al. Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients With Moderate COVID-19: A Randomized Clinical Trial. JAMA 2020; 324(11): 1048-57.
- Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020; 395(10236): 1569-78.
- Goldman JD, Lye DCB, Hui DS, et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N Engl J Med 2020; 383: 1827-37.
- Goldman DL, Aldrich ML, Hagmann SHF, et al. Compassionate Use of Remdesivir in Children With Severe COVID-19. Pediatrics 2021; 147(5).
- Gilead Sciences, Inc. Study to Evaluate the Safety, Tolerability, Pharmacokinetics, and Efficacy of Remdesivir (GS-5734™) in Participants From Birth to < 18 Years of Age With Coronavirus Disease 2019 (COVID-19) (CARAVAN). Available at: https://www.clinicaltrials.gov/ct2/show/NCT04431453. Accessed 18 November 2020.
- Borrell B. New York clinical trial quietly tests heartburn remedy against coronavirus. Available at: https://www.sciencemag.org/news/2020/04/new-york-clinical-trial-quietly-tests-heartburn-remedy-against-coronavirus.
- Wu C, Liu Y, Yang Y, et al. Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods. Acta Pharm Sin B 2020.
- Freedberg DE, Conigliaro J, Wang TC, et al. Famotidine use is associated with improved clinical outcomes in hospitalized COVID-19 patients: A propensity score matched retrospective cohort study. Gastroenterology 2020; 159(3): 1129-31.
- Baum A, Ajithdoss D, Copin R, et al. REGN-COV2 antibodies prevent and treat SARS-CoV-2 infection in rhesus macaques and hamsters. Science 2020.
- U.S. Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency Use Authorization (EUA) of Bamlanivimab. Available at: https://www.fda.gov/media/143603/download. Accessed 15 November 2020.
- U.S. Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency Use Authorization (EUA) of Casirivimab and Imdevimab. Available at: https://www.fda.gov/media/143892/download. Accessed 9 April 2021.
- U.S. Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency Use Authorization (EUA) of Bamlanivimab and Etesevimab. Available at: https://www.fda.gov/media/145802/download. Accessed 9 April 2021.
- ACTIV-3/TICO LY-CoV555 Study Group, Grund B, Barkauskas CE, et al. A Neutralizing Monoclonal Antibody for Hospitalized Patients with Covid-19. N Engl J Med 2020: [Epub ahead of print 22 December 2020].
- Chen P, Nirula A, Heller B, et al. SARS-CoV-2 Neutralizing Antibody LY-CoV555 in Outpatients with Covid-19. N Engl J Med 2021; 384(3): 229-37.
- Weinreich DM, Sivapalasingam S, Norton T, et al. REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with Covid-19. N Engl J Med 2021; 384(3): 238-51.
- Dougan M, Nirula A, Azizad M, et al. The Impact of Bamlanivimab + Etesevimab Neutralizing Antibody Combination Treatment on Hospitalization Rates and Deaths Among High-Risk Patients Presenting With Mild-to-Moderate COVID-19 Illness. 2021: [Under review].
- Gottlieb RL, Nirula A, Chen P, et al. Effect of Bamlanivimab as Monotherapy or in Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA 2021; 325(7): 632-44.
- Regeneron Pharmaceuticals, Inc. Phase 3 Trial Shows Regen-CoV™ (Casirivimab with Imdevimab) Antibody Cocktail Reduced Hospitalization or Death by 70% in Non-Hospitalized COVID-19 Patients. Available at: https://investor.regeneron.com/news-releases/news-release-details/phase-3-trial-shows-regen-covtm-casirivimab-imdevimab-antibody. Accessed 9 April 2021.
- Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-surveillance/variant-info.html. Accessed 9 April 2021.
- U.S. Food and Drug Administration. Fact Sheet for Health Care Providers: Emergency Use Authorization (EUA) of Regen-CoV™ (casirivimab with imdevimab). Available at: https://www.fda.gov/media/145611/download. Accessed 9 April 2021.
- Jorgensen SCJ, Tse CLY, Burry L, Dresser LD. Baricitinib: A Review of Pharmacology, Safety, and Emerging Clinical Experience in COVID-19. Pharmacotherapy 2020; 40(8): 843-56.
- Bekerman E, Neveu G, Shulla A, et al. Anticancer kinase inhibitors impair intracellular viral trafficking and exert broad-spectrum antiviral effects. J Clin Invest 2017; 127(4): 1338-52.
- Neveu G, Ziv-Av A, Barouch-Bentov R, Berkerman E, Mulholland J, Einav S. AP-2-associated protein kinase 1 and cyclin G-associated kinase regulate hepatitis C virus entry and are potential drug targets. J Virol 2015; 89(8): 4387-404.
- Richardson P, Griffin I, Tucker C, et al. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020; 395(10223): e30-e1.
- Cantini F, Niccoli L, Matarrese D, Nicastri E, Stobbione P, Goletti D. Baricitinib therapy in COVID-19: A pilot study on safety and clinical impact. J Infect 2020; 81(2): 318-56.
- Titanji BK, Farley MM, Mehta A, et al. Use of Baricitinib in Patients with Moderate and Severe COVID-19. Clin Infect Dis 2020.
- Rodriguez-Garcia JL, Sanchez-Nievas G, Arevalo-Serrano J, Garcia-Gomez C, Jimenez-Vizuete JM, Martinez-Alfaro E. Baricitinib improves respiratory function in patients treated with corticosteroids for SARS-CoV-2 pneumonia: an observational cohort study. Rheumatology (Oxford) 2021; 60(1): 399-407.
- Cantini F, Niccoli L, Nannini C, et al. Beneficial impact of Baricitinib in COVID-19 moderate pneumonia; multicentre study. J Infect 2020; 81(4): 647-79.
- Marconi VC, Ramanan AV, de Bono S, et al. Baricitinib plus Standard of Care for Hospitalized Adults with COVID-19. medRxiv 2021: Available at: https://doi.org/10.1101/2021.04.30.21255934 [Preprint 3 May 2021].
- OLUMIANT (baricitinib) tablet, for oral use (package insert). Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207924s000lbl.pdf. Accessed 23 December 2020.
- King B, Maari C, Lain E, et al. Extended Safety Analysis of Baricitinib 2 mg in Adult Patients with Atopic Dermatitis: An Integrated Analysis from Eight Randomized Clinical Trials. Am J Clin Dermatol 2021; 22(3): 395-405.
- Winthrop KL, Harigai M, Genovese MC, et al. Infections in baricitinib clinical trials for patients with active rheumatoid arthritis. Ann Rheum Dis 2020; 79(10): 1290-7.
- Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020; 135(23): 2033-40.
- Kalil AC, Patterson TF, Mehta AK, et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Engl J Med 2021; 384: 795-807.
- Caly L, Druce JD, Catton MG, Jans DA, Wagstaff KM. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Res 2020; 178: 104787.
- Bray M, Rayner C, Noel F, Jans D, Wagstaff K. Ivermectin and COVID-19: A report in Antiviral Research, widespread interest, an FDA warning, two letters to the editor and the authors' responses. Antiviral Res 2020; 178: 104805.
- Ahmed S, Karim MM, Ross AG, et al. A five-day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness. Int J Infect Dis 2020; 103: 214-6.
- Chachar AZK, Khan KA, Asif M, Tanveer K, Khaqan A, Basri R. Effectiveness of Ivermectin in SARS-CoV-2/COVID-19 Patients. Int J Sci 2020; 9(09): 31-5.
- Chaccour C, Casellas A, Blanco-Di Matteo A, et al. The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. EClinicalMedicine 2021; 32: 100720.
- Gorial FI, Mashhadani S, Sayaly HM, et al. Effectiveness of ivermectin as add-on therapy in COVID-19 management (pilot trial). medRxiv 2020: Available at: https://doi.org/10.1101/2020.07.07.20145979 [Epub ahead of print 8 July 2020].
- Hashim HA, Maulood MF, Rasheed AM, Fatak DF, Kabah KK, Abdulamir AS. Controlled randomized clinical trial on using Ivermectin with Doxycycline for treating COVID-19 patients in Baghdad, Iraq. medRxiv 2020: Available at: https://doi.org/10.1101/2020.10.26.20219345 [Preprint 27 October 2020].
- Podder CS, Chowdhury N, Sina MI, Ul Haque WMM. Outcome of ivermectin treated mild to moderate COVID-19 cases: a single-centre, open-label, randomised controlled study. IMC J Med SCi 2020; 14(2): 002. [Epub ahead of print 3 September 2020].
- Rajter JC, Sherman MS, Fatteh N, Vogel F, Sacks J, Rajter JJ. Use of Ivermectin Is Associated With Lower Mortality in Hospitalized Patients With Coronavirus Disease 2019: The Ivermectin in COVID Nineteen Study. Chest 2021; 159(1): 85-92.
- Bukhari SKHS, Asghar A, Perveen N, et al. Efficacy of Ivermectin in COVID-19 Patients with Mild to Moderate Disease. medRxiv 2021: Available at: https://doi.org/10.1101/2021.02.02.21250840 [Preprint 5 February 2021].
- Ravikirti, Roy R, Pattadar C, et al. Ivermectin as a potential treatment for mild to moderate COVID-19–A double blind randomized placebo-controlled trial. medRxiv 2021: Available at: https://doi.org/10.1101/2021.01.05.21249310 [Preprint 9 January 2021].
- Lopez-Medina E, Lopez P, Hurtado IC, et al. Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial. JAMA 2021; 325(14): 1426-35.
- Pott-Junior H, Bastos Paoliello MM, Miguel AQC, et al. Use of ivermectin in the treatment of Covid-19: A pilot trial. Toxicol Rep 2021; 8: 505-10.
- Mohan A, Tiwari P, Suri T, Mittal S, Patel AA, Jain A. Ivermectin in mild and moderate COVID-19 (RIVET-COV): a randomized, placebo-controlled trial. Research Square 2021: Available at: https://doi.org/10.21203/rs.3.rs-191648/v1 [Preprint 2 February 2021].
- Babalola OE, Bode CO, Ajayi AA, et al. Ivermectin shows clinical benefits in mild to moderate Covid19 disease: A randomised controlled double blind dose response study in Lagos. medRxiv 2021: Available at: https://doi.org/10.1101/2021.01.05.21249131 [Preprint 6 January 2021].
- Elgazzar A, Hany B, Youssef SA, Hafez M, Moussa H. Efficacy and Safety of Ivermectin for Treatment and prophylaxis of COVID-19 Pandemic. 2020: Available at: https://doi.org/10.21203/rs.3.rs-100956/v1 [Preprint 28 December 2020].
- Niaee MS, Gheibi N, Namdar P, et al. Ivermectin as an adjunct treatment for hospitalized adult COVID-19 patients: A randomized multi-center clinical trial. 2020: Available at: https://doi.org/10.21203/rs.3.rs-109670/v1 [Preprint 24 November 2020].
- Rezaie S. COVID-19 Update: Ivermectin. Available at: https://rebelem.com/covid-19-update-ivermectin/. Accessed 10 February 2021.
- Shoumann WM, Hegazy AA, Nafae RM, et al. Use of Ivermectin as a Potential Chemoprophylaxis for COVID-19 in Egypt: A Randomized Clinical Trial. JCDR 2021; 15(2): OC27-OC32.
- Peral de Bruno MdlA, Chala RE. Prophylaxis Covid-19 in Healthcare Agents by Intensive Treatment With Ivermectin and Iota-carrageenan (Ivercar-Tuc). Available at: https://clinicaltrials.gov/ct2/show/NCT04701710.
- Raad H. In vivo use of ivermectin (IVR) for treatment for corona virus infected patients (COVID-19): a randomized controlled trial. Available at: http://www.chictr.org.cn/showprojen.aspx?proj=54707.
- Mahmud R. Clinical Trial of Ivermectin Plus Doxycycline for the Treatment of Confirmed Covid-19 Infection. Available at: https://clinicaltrials.gov/ct2/show/NCT04523831.
- Lu H. Efficacy and Safety of Darunavir and Cobicistat for Treatment of Pneumonia Caused by 2019-nCoV (DACO-nCoV). Available at: https://clinicaltrials.gov/ct2/show/NCT04252274?id=NCT04252274.
- Chan JF, Chan KH, Kao RY, et al. Broad-spectrum antivirals for the emerging Middle East respiratory syndrome coronavirus. J Infect 2013; 67(6): 606-16.
- Kim JW, Kim EJ, Kwon HH, et al. Lopinavir-ritonavir versus hydroxychloroquine for viral clearance and clinical improvement in patients with mild to moderate coronavirus disease 2019. Korean J Intern Med 2020.
- Zhu Z, Lu Z, Xu T, et al. Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19. J Infect 2020; 81(1): e21-e3.
- Davoudi-Monfared E, Rahmani H, Khalili H, et al. Efficacy and safety of interferon beta-1a in treatment of severe COVID-19: A randomized clinical trial. medRxiv 2020.
- Holland HK, Bashey A, Morris L, E, Solomon S, Solh M. Use of Convalescent Plasma for COVID-19. Available at: https://clinicaltrials.gov/ct2/show/NCT04408040.
- Justman JE, Zech J. Convalescent Plasma for COVID-19 Close Contacts. Available at: https://clinicaltrials.gov/ct2/show/NCT04390503.
- Mohamed MA, El Ekiaby M, Ez-Eldin AM, Hussein AM, Selim AM. Clinical Study for Efficacy of Anti-Corona VS2 Immunoglobulins Prepared From COVID19 Convalescent Plasma Prepared by VIPS Mini-Pool IVIG Medical Devices in Prevention of SARS-CoV-2 Infection in High Risk Groups as Well as Treatment of Early Cases of COVID19 Patients. Available at: https://clinicaltrials.gov/ct2/show/NCT04383548.
- Johns Hopkins University, Jain SK, Gordon O. Human Convalescent Plasma for High Risk Children Exposed or Infected With SARS-CoV-2 (COVID-19). Available at: https://clinicaltrials.gov/ct2/show/NCT04377672.
- Shoham S. Efficacy and Safety Human Coronavirus Immune Plasma (HCIP) vs. Control (SARS-CoV-2 Non-immune Plasma) Among Adults Exposed to COVID-19 (CSSC-001). Available at: https://clinicaltrials.gov/ct2/show/NCT04323800.
- Bloch EM, Shoham S, Casadevall A, et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J Clin Invest 2020; 130(6): 2757-65.
- The IMpact-RSV Study Group. Palivizumab, a Humanized Respiratory Syncytial Virus Monoclonal Antibody, Reduces Hospitalization From Respiratory Syncytial Virus Infection in High-risk Infants. Pediatrics 1998; 102(3): 531-7.
- Feltes TF, Cabalka AK, Meissner HC, et al. Palivizumab prophylaxis reduces hospitalization due to respiratory syncytial virus in young children with hemodynamically significant congenital heart disease. J Pediatr 2003; 143(4): 532-40.
- ter Meulen J, Bakker AB, van den Brink EN, et al. Human monoclonal antibody as prophylaxis for SARS coronavirus infection in ferrets. Lancet 2004; 363(9427): 2139-41.
- Stockman LJ, Bellamy R, Garner P. SARS: systematic review of treatment effects. PLoS Med 2006; 3(9): e343.
- Arabi YM, Shalhoub S, Mandourah Y, et al. Ribavirin and Interferon Therapy for Critically Ill Patients With Middle East Respiratory Syndrome: A Multicenter Observational Study. Clin Infect Dis 2019.
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020; 395(10223): 507-13.
- Ning Q, Han M. A Prospective/Retrospective, Randomized Controlled Clinical Study of Antiviral Therapy in the 2019-nCoV Pneumonia. Available at: https://clinicaltrials.gov/ct2/show/NCT04255017.
- Ning Q, Han M. A Randomized, Open, Controlled Clinical Study to Evaluate the Efficacy of ASC09F and Ritonavir for 2019-nCoV Pneumonia. Available at: https://clinicaltrials.gov/ct2/show/NCT04261270.
- Kongsaengdao S, Sawanpanyalert N. Various Combination of Protease Inhibitors, Oseltamivir, Favipiravir, and Hydroxychloroquine for Treatment of COVID19 : A Randomized Control Trial (THDMS-COVID19). Available at: https://clinicaltrials.gov/ct2/show/NCT04303299.
- Cao W, Liu X, Bai T, et al. High-Dose Intravenous Immunoglobulin as a Therapeutic Option for Deteriorating Patients With Coronavirus Disease 2019. Open Forum Infect Dis 2020; 7(3): ofaa102.
- Sakoulas G, Geriak M, Kullar R, et al. Intravenous Immunoglobulin (IVIG) Significantly Reduces Respiratory Morbidity in COVID-19 Pneumonia: A Prospective Randomized Trial. medRxiv 2020.
- Xie Y, Cao S, Dong H, et al. Effect of regular intravenous immunoglobulin therapy on prognosis of severe pneumonia in patients with COVID-19. J Infect 2020; 81(2): 318-56.
- Mohtadi N, Ghaysouri A, Shirazi S, et al. Recovery of severely ill COVID-19 patients by intravenous immunoglobulin (IVIG) treatment: A case series. Virology 2020; 548: 1-5.
- Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020; 181(2): 271-80 e8.
- Coxib, traditional NTC, Bhala N, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet 2013; 382(9894): 769-79.
- Zhang X, Donnan PT, Bell S, Guthrie B. Non-steroidal anti-inflammatory drug induced acute kidney injury in the community dwelling general population and people with chronic kidney disease: systematic review and meta-analysis. BMC Nephrol 2017; 18(1): 256.
- Voiriot G, Dury S, Parrot A, Mayaud C, Fartoukh M. Nonsteroidal antiinflammatory drugs may affect the presentation and course of community-acquired pneumonia. Chest 2011; 139(2): 387-94.
- Voiriot G, Philippot Q, Elabbadi A, Elbim C, Chalumeau M, Fartoukh M. Risks Related to the Use of Non-Steroidal Anti-Inflammatory Drugs in Community-Acquired Pneumonia in Adult and Pediatric Patients. J Clin Med 2019; 8(6).
- Mancia G, Rea F, Ludergnani M, Apolone G, Corrao G. Renin-Angiotensin-Aldosterone System Blockers and the Risk of Covid-19. N Engl J Med 2020; 382(25): 2431-40.
- World Health Organization. The use of non-steroidal anti-inflammatory drugs (NSAIDs) in patients with COVID-19. Available at: https://www.who.int/news-room/commentaries/detail/the-use-of-non-steroidal-anti-inflammatory-drugs-(nsaids)-in-patients-with-covid-19. Accessed 18 June 2020.
- Castro VM, Ross RA, McBride SM, Perlis RH. Identifying common pharmacotherapies associated with reduced COVID-19 morbidity using electronic health records. medRxiv 2020.
- Adnet F, Slama Schwok A. Efficacy of Addition of Naproxen in the Treatment of Critically Ill Patients Hospitalized for COVID-19 Infection (ENACOVID). Available at: https://clinicaltrials.gov/ct2/show/NCT04325633.
- Beale R, Mazibuko N, Farrell C, King's College London. LIBERATE Trial in COVID-19 (LIBERATE). Available at: https://clinicaltrials.gov/ct2/show/NCT04334629.
- Vaduganathan M, Vardeny O, Michel T, McMurray JJV, Pfeffer MA, Solomon SD. Renin-Angiotensin-Aldosterone System Inhibitors in Patients with Covid-19. N Engl J Med 2020; 382(17): 1653-9.
- Ferrario CM, Jessup J, Chappell MC, et al. Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation 2005; 111(20): 2605-10.
- Ishiyama Y, Gallagher PE, Averill DB, Tallant EA, Brosnihan KB, Ferrario CM. Upregulation of angiotensin-converting enzyme 2 after myocardial infarction by blockade of angiotensin II receptors. Hypertension 2004; 43(5): 970-6.
- Dijkman R, Jebbink MF, Deijs M, et al. Replication-dependent downregulation of cellular angiotensin-converting enzyme 2 protein expression by human coronavirus NL63. J Gen Virol 2012; 93(Pt 9): 1924-9.
- Sodhi CP, Wohlford-Lenane C, Yamaguchi Y, et al. Attenuation of pulmonary ACE2 activity impairs inactivation of des-Arg(9) bradykinin/BKB1R axis and facilitates LPS-induced neutrophil infiltration. Am J Physiol Lung Cell Mol Physiol 2018; 314(1): L17-L31.
- Zhang P, Zhu L, Cai J, et al. Association of Inpatient Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers With Mortality Among Patients With Hypertension Hospitalized With COVID-19. Circ Res 2020; 126(12): 1671-81.
- Li J, Wang X, Chen J, Zhang H, Deng A. Association of Renin-Angiotensin System Inhibitors With Severity or Risk of Death in Patients With Hypertension Hospitalized for Coronavirus Disease 2019 (COVID-19) Infection in Wuhan, China. JAMA Cardiol 2020.
- Bean DM, Kraljevic Z, Searle T, et al. Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are not associated with severe COVID-19 infection in a multi-site UK acute hospital trust. Eur J Heart Fail 2020; 22(6): 967-74.
- Tedeschi S, Giannella M, Bartoletti M, et al. Clinical Impact of Renin-angiotensin System Inhibitors on In-hospital Mortality of Patients With Hypertension Hospitalized for Coronavirus Disease 2019. Clin Infect Dis 2020; 71(15): 899-901.
- Reynolds HR, Adhikari S, Pulgarin C, et al. Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Covid-19. N Engl J Med 2020; 382(25): 2441-8.
- Fosbol EL, Butt JH, Ostergaard L, et al. Association of Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use With COVID-19 Diagnosis and Mortality. JAMA 2020.
- Oussalah A, Gleye S, Clerc Urmes I, et al. Long-Term ACE Inhibitor/ARB Use Is Associated with Severe Renal Dysfunction and Acute Kidney Injury in Patients with severe COVID-19: Results from a Referral Center Cohort in the North East of France. Clin Infect Dis 2020.
- European Society of Cardiology. Position Statement of the ESC Council on Hypertension on ACE-Inhibitors and Angiotensin Receptor Blockers. Available at: https://www.escardio.org/Councils/Council-on-Hypertension-(CHT)/News/position-statement-of-the-esc-council-on-hypertension-on-ace-inhibitors-and-ang. Accessed 3 August 2020.
- Association AH. Patients taking ACE-i and ARBs who contract COVID-19 should continue treatment, unless otherwise advised by their physician. Available at: https://newsroom.heart.org/news/patients-taking-ace-i-and-arbs-who-contract-covid-19-should-continue-treatment-unless-otherwise-advised-by-their-physician. Accessed 3 August 2020.
- International Society of Hypertension. A statement from the International Society of Hypertension on COVID-19. Available at: https://ish-world.com/news/a/A-statement-from-the-International-Society-of-Hypertension-on-COVID-19. Accessed 3 August 2020.
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020; 395(10229): 1054-62.
- Rojo JMC, Santos JMA, Núñez-Cortés JM, et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: results from the SEMI-COVID-19 Network. medRxiv 2020.
- Argenziano MG, Bruce SL, Slater CL, et al. Characterization and clinical course of 1000 Patients with COVID-19 in New York: retrospective case series. medRxiv 2020.
- Rawson TM, Moore LSP, Zhu N, et al. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin Infect Dis 2020.
- Goyal P, Choi JJ, Pinheiro LC, et al. Clinical Characteristics of Covid-19 in New York City. N Engl J Med 2020; 382(24): 2372-4.
- Sepulveda J, Westblade LF, Whittier S, et al. Bacteremia and Blood Culture Utilization during COVID-19 Surge in New York City. Journal of clinical microbiology 2020; 58(8).
- Wei W, Ortwine JK, Mang NS, Joseph C, Hall BC, Prokesch BC. Limited Role for Antibiotics in COVID-19: Scarce Evidence of Bacterial Coinfection. Available at SSRN 3622388 2020.
- McCreary EK, Pogue JM. Coronavirus Disease 2019 Treatment: A Review of Early and Emerging Options. Open Forum Infect Dis 2020; 7(4): ofaa105.
- Clancy CJ, Nguyen MH. COVID-19, superinfections and antimicrobial development: What can we expect? Clin Infect Dis 2020.
- Furuta Y, Gowen BB, Takahashi K, Shiraki K, Smee DF, Barnard DL. Favipiravir (T-705), a novel viral RNA polymerase inhibitor. Antiviral Res 2013; 100(2): 446-54.
- Cai Q, Yang M, Liu D, et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering (Beijing) 2020.
- Chen C, Huang J, Cheng Z, et al. Favipiravir versus arbidol for COVID-19: a randomized clinical trial. MedRxiv 2020.
- Lou Y, Liu L, Qiu Y. Clinical Outcomes and Plasma Concentrations of Baloxavir Marboxil and Favipiravir in COVID-19 Patients: an Exploratory Randomized, Controlled Trial. medRxiv 2020.
- Cavalli G, De Luca G, Campochiaro C, et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: a retrospective cohort study. Lancet Rheumatol 2020; 2(6): e325-e31.
- Chatham WW, Kendrach A, University of Alabama at Birmingham. Early Identification and Treatment of Cytokine Storm Syndrome in Covid-19. Available at: https://www.clinicaltrials.gov/ct2/show/NCT04362111.
- Ucciferri C, Auricchio A, Di Nicola M, et al. Canakinumab in a subgroup of patients with COVID-19. Lancet Rheumatol 2020; 2(8): e457-ee8.
- Novartis Pharamaceuticals. Study of Efficacy and Safety of Canakinumab Treatment for CRS in Participants With COVID-19-induced Pneumonia (CAN-COVID). Available at: https://clinicaltrials.gov/ct2/show/NCT04362813.
- National Institute of Allergy and Infectious Diseases (NIAID). Adaptive COVID-19 Treatment Trial 2 (ACTT-2). Available at: https://clinicaltrials.gov/ct2/show/NCT04401579.
- Hall F. mulTi-Arm Therapeutic Study in Pre-ICu Patients Admitted With Covid-19 - Repurposed Drugs (TACTIC-R) (TACTIC-R). Available at: https://clinicaltrials.gov/ct2/show/NCT04390464.
- Eli Lilly and Company. A Study of Baricitinib (LY3009104) in Participants With COVID-19 (COV-BARRIER). Available at: https://clinicaltrials.gov/ct2/show/NCT04421027.
- Lenz H-J, University of Southern California. Baricitinib, Placebo and Antiviral Therapy for the Treatment of Patients With Moderate and Severe COVID-19. Available at: https://clinicaltrials.gov/ct2/show/NCT04373044.
- Menichetti F, Ospedaliero A. Baricitinib Compared to Standard Therapy in Patients With COVID-19 (BARICIVID-19). Available at: https://clinicaltrials.gov/ct2/show/NCT04393051.
- De Luca G, Cavalli G, Campochiaro C, et al. GM-CSF blockade with mavrilimumab in severe COVID-19 pneumonia and systemic hyperinflammation: a single-centre, prospective cohort study. Lancet Rheumatol 2020; 2(8): e465-e73.
- Durrant C, Ahmed O, Humanigen, Inc. Phase 3 Study to Evaluate Efficacy and Safety of Lenzilumab in Patients With COVID-19. Available at: https://clinicaltrials.gov/ct2/show/NCT04351152.
- Xu C, Kumar P, Siegel M, et al. Study of TJ003234 (Anti-GM-CSF Monoclonal Antibody) in Subjects With Severe Coronavirus Disease 2019 (COVID-19). Available at: https://www.clinicaltrials.gov/ct2/show/NCT04341116.
- Dagna L, De Luca G, Ospedale San Raffaele. Mavrilimumab in Severe COVID-19 Pneumonia and Hyper-inflammation (COMBAT-19) (COMBAT-19). Available at: https://clinicaltrials.gov/ct2/show/NCT04397497.
- Bergeron-Lafaurie A, Azoulay E, Peffault de Latour R, Assistance Publique - Hôpitaux de Paris. CORIMUNO19-ECU: Trial Evaluating Efficacy and Safety of Eculizumab (Soliris) in Patients With COVID-19 Infection, Nested in the CORIMUNO-19 Cohort (CORIMUNO19-ECU). Available at: https://clinicaltrials.gov/ct2/show/NCT04346797.
- Dong Y, Mo X, Hu Y, et al. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020; 145(6).
- Kim L, Whitaker M, O'Halloran A, et al. Hospitalization Rates and Characteristics of Children Aged <18 Years Hospitalized with Laboratory-Confirmed COVID-19 - COVID-NET, 14 States, March 1-July 25, 2020. MMWR Morb Mortal Wkly Rep 2020; 69(32): 1081-8.
- Shekerdemian LS, Mahmood NR, Wolfe KK, et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr 2020.
- National Institute of Allergy and Infectious Diseases (NIAID). Adaptive COVID-19 Treatment Trial (ACTT). Available at: https://clinicaltrials.gov/ct2/show/NCT04280705.
- Gilead Sciences, Inc. Study to Evaluate the Safety and Antiviral Activity of Remdesivir (GS-5734™) in Participants With Severe Coronavirus Disease (COVID-19). Available at: https://clinicaltrials.gov/ct2/show/NCT04292899.
- Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 - Preliminary Report. N Engl J Med 2020.
- U.S. Food and Drug Administration. Letter of FDA Emergency Use Authorization to Ashley Rhodes dated May 1, 2020. In: Rhoades A, Gilead Sciences, Inc., 2020.
- Belhadjer Z, Méot M, Bajolle F, et al. Acute heart failure in multisystem inflammatory syndrome in children (MIS-C) in the context of global SARS-CoV-2 pandemic. Circulation 2020; 142(5): 429-36.
- Deza Leon MP, Redzepi A, McGrath E, et al. COVID-19-Associated Pediatric Multisystem Inflammatory Syndrome. J Pediatric Infect Dis Soc 2020; 9(3): 407-8.
- Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet (London, England) 2020; 395(10237): 1607-8.
- Verdoni L, Mazza A, Gervasoni A, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. The Lancet 2020; 395(10239): 1771-8.
- Blondiaux E, Parisot P, Redheuil A, et al. Cardiac MRI of Children with Multisystem Inflammatory Syndrome (MIS-C) Associated with COVID-19: Case Series. Radiology 2020: 202288.
- Greene AG, Saleh M, Roseman E, Sinert R. Toxic shock-like syndrome and COVID-19: A case report of multisystem inflammatory syndrome in children (MIS-C). Am J Emerg Med 2020.
- Pouletty M, Borocco C, Ouldali N, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort. Ann Rheum Dis 2020; 79(8): 999-1006.
- Chiotos K, Bassiri H, Behrens EM, et al. Multisystem Inflammatory Syndrome in Children During the Coronavirus 2019 Pandemic: A Case Series. J Pediatric Infect Dis Soc 2020; 9(3): 393-8.
- Cabrero-Hernandez M, Garcia-Salido A, Leoz-Gordillo I, et al. Severe SARS-CoV-2 Infection in Children With Suspected Acute Abdomen: A Case Series From a Tertiary Hospital in Spain. Pediatr Infect Dis J 2020; 39(8): e195-e8.
- Feldstein LR, Rose EB, Horwitz SM, et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med 2020; 383(4): 334-46.
- Dufort EM, Koumans EH, Chow EJ, et al. Multisystem Inflammatory Syndrome in Children in New York State. New England Journal of Medicine 2020.
- Whittaker E, Bamford A, Kenny J, et al. Clinical Characteristics of 58 Children With a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA 2020; 324(3): 259-69.
- Godfred-Cato S, Bryant B, Leung J, et al. COVID-19-Associated Multisystem Inflammatory Syndrome in Children - United States, March-July 2020. MMWR Morb Mortal Wkly Rep 2020; 69(32): 1074-80.
- Centers for Disease Control and Prevention. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). Available at: https://emergency.cdc.gov/han/2020/han00432.asp. Accessed 24 May 2020.
- Royal College of Paediatrics and Child Health. Guidance: Paediatric multisystem inflammatory syndrome temporally associated with COVID-19, 2020.
- Rowley AH. Understanding SARS-CoV-2-related multisystem inflammatory syndrome in children. Nat Rev Immunol 2020; 20(8): 453-4.
- Diorio C, Henrickson SE, Vella LA, et al. Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS-CoV-2. J Clin Invest 2020.
- Kalil AC. Treating COVID-19-Off-Label Drug Use, Compassionate Use, and Randomized Clinical Trials During Pandemics. JAMA 2020.
- Bauchner H, Golub RM, Zylke J. Editorial Concern-Possible Reporting of the Same Patients With COVID-19 in Different Reports. JAMA 2020.
- Zhao R, Wang H, Wang X, Feng F. Steroid therapy and the risk of osteonecrosis in SARS patients: a dose-response meta-analysis. Osteoporos Int 2017; 28(3): 1027-34.
- Calain P. The Ebola clinical trials: a precedent for research ethics in disasters. J Med Ethics 2018; 44(1): 3-8.
- Cook D, Burns K, Finfer S, et al. Clinical research ethics for critically ill patients: a pandemic proposal. Crit Care Med 2010; 38(4 Suppl): e138-42.
- Fowler RA, Webb SA, Rowan KM, et al. Early observational research and registries during the 2009-2010 influenza A pandemic. Crit Care Med 2010; 38(4 Suppl): e120-32.
- Iwashyna TJ, McPeake J. Choosing outcomes for clinical trials: a pragmatic perspective. Curr Opin Crit Care 2018; 24(5): 428-33.