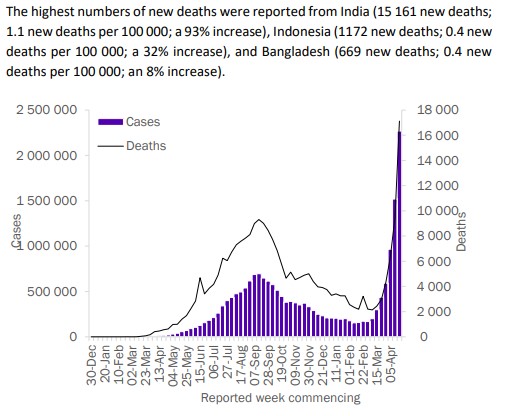
On April 27 the World Health Organization included in its very helpful weekly epidemiological update on COVID-19 a section on variants, including the one termed “B.1.617” (formerly mis-termed “double mutant”). WHO placed into context the rapidly rising numbers of cases in India with the lower and decreasing numbers of cases in the USA and Brazil: “The highest numbers of new cases were reported from India (2 172 063 new cases; 52% increase), the United States of America (406 001 new cases; 15% decrease), Brazil (404 623 new cases; 12% decrease) . . .”
In addition, the stunning graph and text below regarding deaths and cases in India within the context of the nations in the WHO Southeast Asia region are cited verbatim from data as presented on page 12 of this 30-page pdf document.
Although an imperfect analogy, this second wave of pandemic COVID-19 in India brought to mind reading about the autumn 1918 second wave of pandemic influenza in the United States. John Barry’s masterpiece book The Great Influenza has a section (VIII) titled “Tolling of the Bell”. In chapter 28 he described in detail the overwhelming conditions in Philadelphia in September through October of 1918. For example, on page 326-327 of the 2009 edition he writes of the effect of the abrupt rise in the numbers of deaths: “The corpses had backed up at undertakers’, filling every area of these establishments and pressing up into living quarters; in hospital morgues overflowing into corridors; in the city morgue overflowing into the street. And they had backed up in homes . . .”
Chapter 29, the next chapter, begins “What was happening in Philadelphia was happening everywhere…”
Without further comment, the WHO update on this B.1.617 variant is copied below for interested readers:
“Variants of interest B.1.617
“Emerging SARS-CoV-2 variants within Pango lineage B.1.617 were recently reported as a VOI from India and has recently been designated as VOIs by WHO. As of 27 April, over 1200 sequences have been uploaded to GISAID and assigned to lineage B.1.617 (collectively) from at least 17 countries; most sequences were uploaded from India, the United Kingdom, USA and Singapore. However, this lineage comprises several sub-lineages, including B.1.617.1, B.1.617.2 and B.1.617.3, which slightly differ by their characteristic mutations. Both B.1.617.1 and B.1.617.2 were first identified in India in December 2020, and have been detected at increasing prevalence concurrent to the major upsurge observed in the country. B.1.617.3 was first detected in India in October 2020, but relatively fewer viruses matching this sub-lineage have been reported to date.
"B.1.617 includes several mutations present in other VOIs / VOCs that have been associated with phenotypic impacts. Three characteristic mutations of this variant include L452R, P681R, and E484Q (the latter observed in sub-lineages B.1.617.1 and B.1.617.3). L452R has been identified in another VOI, B.1.427/ B.1.429, which has been associated with increased transmissibility, a reduction in neutralization by some (but not all) monoclonal antibody treatments, and a moderate reduction in neutralization in post-vaccination sera in the USA.46 P681R is adjacent to the furin cleavage site, and (together with other mutations) may enhance binding and subsequent cleavage of the spike protein and enhances systemic infection and membrane fusion; potentially resulting in enhanced transmission.47 Laboratory studies suggest that convalescent samples from individuals who had natural infection may have reduced neutralization against variants with an E484Q mutation.48 Preliminary laboratory studies of a small number of convalescent sera samples of COVID-19 cases (n=17) and recipients of Novavax-Covaxin (n=28) were able to neutralize B.1.617.49.
"In India, heterogeneity in B.1.617 geographic distribution is observed across regions, with co-circulation of other VOCs (including VOC 202012/01 and 501Y.V2) and other variants (e.g., B.1.618), which collectively may be playing a role in the current resurgence in this country. Indeed, studies have highlighted that the spread of the second wave has been much faster than the first. Preliminary modelling by WHO based on sequences submitted to GISAID suggest that B.1.617 has a higher growth rate than other circulating variants in India, suggesting potential increased transmissibility, with other co-circulating variants also demonstrating increased transmissibility. Other drivers may include challenges around the implementation and adherence to public health and social measures (PHSM), and social gatherings (including mass gatherings during cultural and religious celebrations, and elections). Further investigation is needed to understand the relative contribution of these factors.
"It remains unclear how generalizable laboratory-based studies of limited sample sizes, as well as studies of other variants with similar key mutations, are to the wider circulating B.1.617 variants. Further robust studies into the phenotypic impacts of these variants, including impacts on epidemiological characteristics (transmissibility, severity, reinfection risk, etc.) and impact on countermeasures, are urgently needed.”