Last Updated:
July 06, 2026 This Has Been Corrected / Updated. View Update HistoryAuthors:
Mindy G. Schuster*, C. Orla Morrissey*, Shahid Husain, M. Hong Nguyen, Nitipong Permpalung, Jo-Anne H. Young, Aadith Ashok, David R. Andes, Monica I. Ardura, Antonio C. Arrieta, Eric J. Bow, Pranatharthi H. Chandrasekar, Sharon C-A. Chen, Sarah P. Hammond, Sophia A. Koo, Thomas F. Patterson, Miranda So, George R. Thompson, Valéry LavergneRelated Content:
IDSA 2016 Clinical Practice Guideline Update for the Diagnosis and Management of AspergillosisBackground
Invasive aspergillosis (IA) remains a significant cause of morbidity and mortality in immunocompromised patients. The previous Infectious Disease Society of America (IDSA) Practice Guideline for the Diagnosis and Management of Aspergillosis was published in 2016 [1]. The purpose of these updated guidelines is to provide evidence-based reviews and guidance for practitioners managing adult patients at-risk for or with suspected or documented Aspergillus spp. infections.
This first section addresses antifungal prophylaxis for IA in adult SOT recipients (liver, kidney, pancreas, lung or heart transplant). While antifungal prophylaxis against Candida and Candida-like infections is common post-transplant, these guidelines focus specifically on anti-mold prophylaxis to prevent IA. We examine several strategies including universal prophylaxis, preemptive therapy and targeted prophylaxis (see Table 1 for Definitions), as well as the antifungal agents used for prophylaxis.
Table 1. Definitions of the Different Types of Antifungal Prophylaxis in Solid Organ Transplant Recipients
![]()
Abbreviations: IA, invasive aspergillosis
Methods
The panel included adult and pediatric infectious disease specialists, pharmacology experts, and one microbiologist with expertise in patients at risk for Aspergillus infections. It included members with expertise in hematologic malignancy (HM), hematopoietic cell transplantation (HCT), and solid organ transplantation (SOT). Four expert panelists were partner representatives from the following stakeholder organizations: the American Academy of Pediatrics (AAP), American Society of Clinical Oncology (ASCO), American Society of Transplantation (AST), and the Pediatric Infectious Disease Society (PIDS).
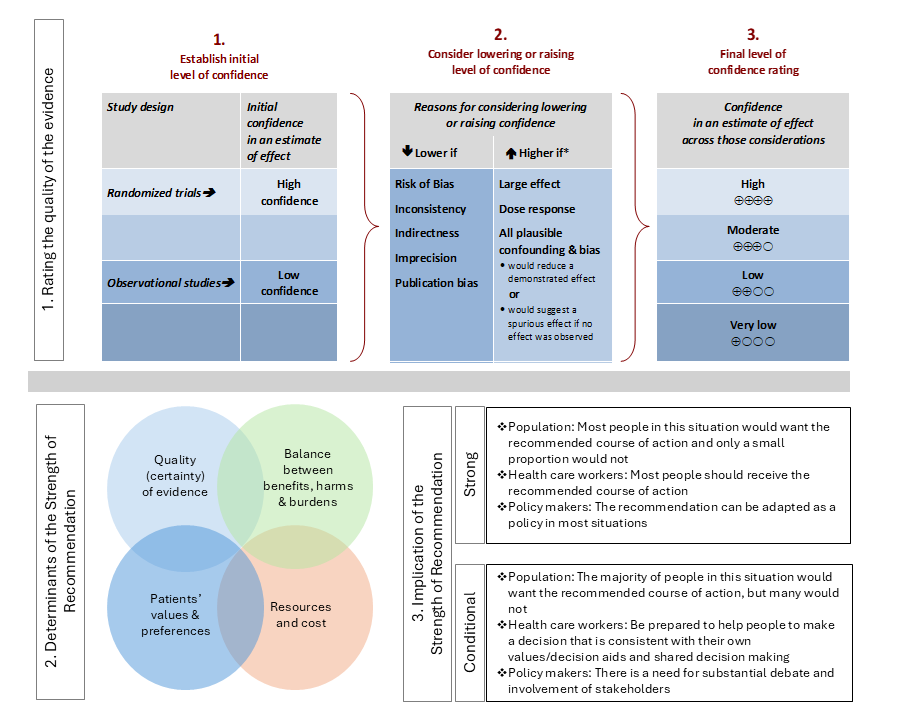
As per the prioritization process, clinical questions for liver and lung transplant populations were selected to be addressed using IDSA guideline methodology to formulate recommendations. For each clinical question, a systematic review was performed to identify relevant studies, and the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach was followed for assessing the certainty of evidence and strength of recommendation (Figure 1).
Additionally, the incidence of IA in the SOT populations not receiving anti-Aspergillus prophylaxis was addressed using a standardized approach to formulate conclusions. For each incidence of IA in a specific subpopulation, a mapping review was performed to identify relevant studies. Details of the literature review and guideline development processes are available in the Methods section and Supplementary materials for each subpopulation.
Figure 1. Approach and Implications to Rating the Quality of Evidence and Strength of Recommendations Using GRADE Methodology (unrestricted use of figure granted by the U.S. GRADE Network)
Recommendations and Conclusions
Liver Transplant Recipients Recommendation 1
In liver transplant recipients, we suggest against using universal anti-Aspergillus prophylaxis (conditional recommendation, low certainty of evidence).
Remarks
- Universal prophylaxis is defined as the administration of prophylaxis to all liver transplant recipients.
- In the included studies, universal anti-Aspergillus prophylaxis (agents examined were anidulafungin, micafungin, itraconazole, and liposomal amphotericin B) was compared with either fluconazole or no antifungal prophylaxis.
- This recommendation places a high value on avoiding adverse events and unnecessary costs, given the lack of clear clinically significant benefits.
Liver Transplant Recipients Recommendation 2
In liver transplant recipients, we suggest targeted anti-Aspergillus prophylaxis for individuals at high risk of invasive aspergillosis (conditional recommendation, very low certainty of evidence).
Remarks
- Targeted prophylaxis refers to antifungal prophylaxis given only to patients who are at high risk for invasive aspergillosis. In the evidence reviewed, the most common risk factors for IA included: 1) renal replacement therapy in the peri-transplantation period, 2) re-transplantation, and 3) transplantation for fulminant hepatic failure.
- In the included study, voriconazole was evaluated as a prophylactic agent in both targeted and universal strategies.
- The duration of anti-Aspergillus prophylaxis in the included evidence was typically until discharge from the initial transplant hospitalization through 28 days post-transplant.
- This recommendation places a high value on balancing potential benefits while improving stewardship and reducing costs.
Liver Transplant Recipients Recommendation 3
In liver transplant recipients requiring anti-Aspergillus prophylaxis, we suggest using an echinocandin or a newer anti-mold triazole (voriconazole, posaconazole or isavuconazole) rather than amphotericin B formulations or itraconazole (conditional recommendation, very low certainty of evidence).
Remarks
- This recommendation prioritizes reducing adverse events (e.g., nephrotoxicity and hepatotoxicity), minimizing drug-drug interactions (especially with cyclosporine, tacrolimus, sirolimus and everolimus), and optimizing bioavailability.
- Among the anti-mold triazoles, the available evidence is derived primarily from studies evaluating voriconazole. To date, no peer-reviewed studies have specifically assessed posaconazole or isavuconazole for prophylaxis in liver transplant recipients. Based on indirect evidence from other transplant populations, these anti-mold triazoles (voriconazole, posaconazole and isavuconazole) are expected to provide comparable benefits.
Kidney Transplant Recipients Conclusion
Given the low pooled incidence of IA, the use of universal anti-Aspergillus prophylaxis is expected to provide limited benefits and thus a less favorable balance of benefits and harms. The current available evidence does not support the use of universal IA prophylaxis in kidney transplant recipients.
Pancreas Transplant Recipients Conclusion
Given the low pooled incidence of IA, the use of universal anti-Aspergillus prophylaxis is expected to provide limited benefits and thus a less favorable balance of benefits and harms. The current available evidence does not support the use of universal IA prophylaxis in pancreas transplant recipients.
Lung Transplant Recipients Recommendation 1
In lung transplant recipients, we make no recommendation for or against universal anti-Aspergillus prophylaxis (no recommendation, knowledge gap).
Remarks
- The panel concluded that the potential benefits of the universal as compared to no anti-Aspergillus prophylaxis remain unclear. There are critical risks of bias in existing studies, unexplored sources of heterogeneity between studies, and serious concerns regarding their lack of generalizability to current clinical practice. Further studies are needed to evaluate the effectiveness and safety of antifungal agents particularly in respect to potential harms such as serious adverse events, drug-drug interactions, costs and challenges related to antimicrobial stewardship.
- The role of antifungal prophylaxis in lung transplantation remains complex due to the lack of high-quality evidence supporting a standardized approach, leading to significant variability in practice. Please refer to the “Considerations When Implementing a Prophylactic Strategy” section.
Lung Transplant Recipients Recommendation 2
In lung transplant recipients, we make no recommendation for or against any targeted anti-Aspergillus prophylaxis or preemptive therapy rather than universal anti-Aspergillus prophylaxis (no recommendation, knowledge gap).
Remarks
- The panel concluded that the potential benefits of the different anti-Aspergillus prophylactic strategies (universal prophylaxis, targeted prophylaxis, and preemptive therapy) remain unclear. There are critical risks of bias in existing studies, unexplored sources of heterogeneity between studies, and serious concerns regarding their lack of generalizability to current clinical practice. Further studies are needed to evaluate the effectiveness and safety of antifungal agents in this setting, particularly in respect to potential harms such as serious adverse events, drug-drug interactions, costs and challenges related to antimicrobial stewardship.
- The role of antifungal prophylaxis in lung transplantation remains complex due to the lack of high-quality evidence supporting a standardized approach, leading to significant variability in practice. Please refer to the “Considerations When Implementing a Prophylactic Strategy” section.
Lung Transplant Recipients Recommendation 3
In lung transplant recipients in whom anti-Aspergillus prophylaxis or preemptive therapy is being considered, clinicians should select agent(s) based on the following factors: adverse events profile, drug-drug interactions, ease of administration and tolerability, associated costs and resources, availability, as well as local epidemiology (good practice statement).
Remarks
- In the absence of direct comparisons between different classes of agents in the reviewed evidence, the panel judged that an individualized approach for selecting anti-Aspergillus prophylaxis (if considered) is preferable.
- Comparison between triazoles is presented in the Table “Comparison of Characteristics, Tolerability and Cost of Anti-Mold Triazoles” and between different formulations of aerosolized amphotericin B in the Table “Comparison of Characteristics, Tolerability and Cost of Three Amphotericin B Formulations Adapted for Aerosolized Administration”.
Heart Transplant Recipients Conclusion
Given the relatively low pooled incidence of IA, the use of universal anti-Aspergillus prophylaxis is likely to offer limited benefits and a less favorable balance of benefits and harms. The current evidence does not support routine universal prophylaxis against IA in heart transplant recipients.
Liver Transplant Recipients
Last Updated:
June 26, 2026Literature Review Conducted:
April 01, 2025This Recommendation Is Endorsed By The American Society of Transplantation (AST) and The Pediatric Infectious Diseases Society (PIDS)
Authors:
M. Hong Nguyen*, Jo-Anne H. Young*, Shahid Husain, Nitipong Permpalung, David R. Andes, Miranda So, Monica I. Ardura, Antonio C. Arrieta, Eric J. Bow, Pranatharthi H. Chandrasekar, Sharon C-A. Chen, Sarah P. Hammond, Sophia A. Koo, Thomas F. Patterson, George R. Thompson, Mindy G. Schuster**, C. Orla Morrissey**, Valéry Lavergne**Recommendations
Clinical Question
In liver transplant recipients, what is the optimal anti-Aspergillus prophylaxis strategy (universal versus targeted versus no prophylaxis)?
Recommendation 1
In liver transplant recipients, we suggest against using universal anti-Aspergillus prophylaxis (conditional recommendation, low certainty of evidence).
Remarks
- Universal prophylaxis is defined as the administration of prophylaxis to all liver transplant recipients.
- In the included studies, universal anti-Aspergillus prophylaxis (agents examined were anidulafungin, micafungin, itraconazole, and liposomal amphotericin B) was compared with either fluconazole or no antifungal prophylaxis.
- This recommendation places a high value on avoiding adverse events and unnecessary costs, given the lack of clear clinically significant benefits.
Results
Universal anti-Aspergillus prophylaxis versus no anti-Aspergillus prophylaxis
Summary of Evidence
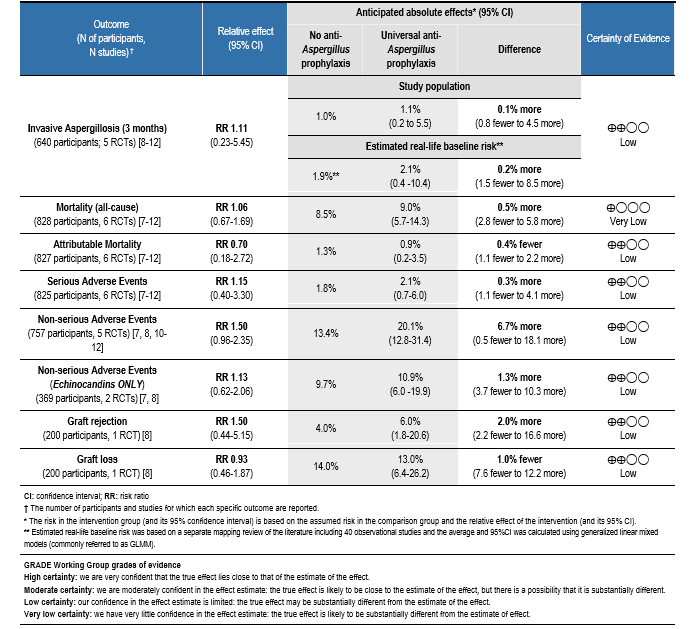
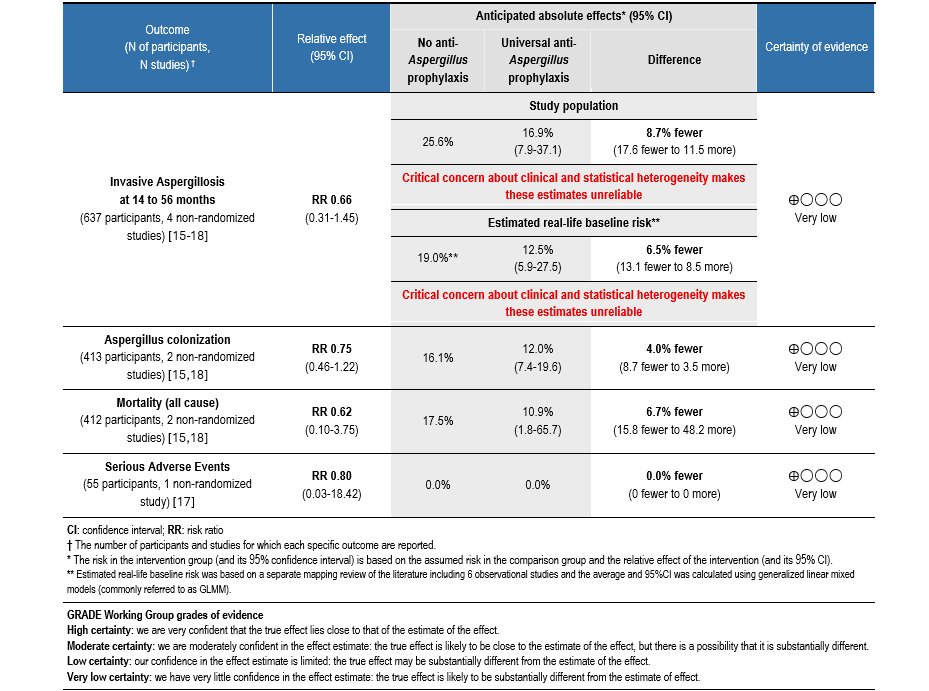
Our systematic review of the literature (spanning from 2000-2025) identified six randomized, controlled trials (RCTs) comparing the use of universal anti-Aspergillus prophylaxis (either anidulafungin, micafungin, itraconazole, or liposomal amphotericin B) with not using anti-Aspergillus prophylaxis (fluconazole or no antifungal prophylaxis) [7-12]. Additionally, to better understand the true burden of IA in liver transplant recipients, a mapping review across 40 observational studies published from 2000 to 2025 was performed to determine the incidence of IA in liver transplant recipients not receiving anti-Aspergillus prophylaxis [8, 11, 12, 15-52].
Table 2. Summary of Findings: Universal Anti-Aspergillus Prophylaxis Versus No Anti-Aspergillus Prophylaxis in Liver Transplant Recipients
Rationale for Recommendation
The use of universal anti-Aspergillus prophylaxis in liver transplant recipients results in comparable desirable and undesirable outcomes to those observed without anti-Aspergillus prophylaxis. The panel agreed that the overall certainty of the evidence for using universal anti-Aspergillus prophylaxis in liver transplant recipients is low. Concerns include potential risks of bias and imprecision due to the low number of reported events. In the absence of demonstrable clinical benefits, the panel concluded that additional harms or drug interactions, together with resource use and cost, weigh against the use of universal anti-Aspergillus prophylaxis in liver transplant recipients. The guideline panel suggested against the use of universal anti-Aspergillus prophylaxis for liver transplant recipients following transplantation.
Recommendation 2
In liver transplant recipients, we suggest targeted anti-Aspergillus prophylaxis for individuals at high risk of invasive aspergillosis (conditional recommendation, very low certainty of evidence).
Remarks
- Targeted prophylaxis refers to antifungal prophylaxis given only to patients who are at high risk for invasive aspergillosis. In the evidence reviewed, the most common risk factors for IA included: 1) renal replacement therapy in the peri-transplantation period, 2) re-transplantation, and 3) transplantation for fulminant hepatic failure.
- In the included study, voriconazole was evaluated as a prophylactic agent in both targeted and universal strategies.
- The duration of anti-Aspergillus prophylaxis in the included evidence was typically until discharge from the initial transplant hospitalization through 28 days post-transplant.
- This recommendation places a high value on balancing potential benefits while improving stewardship and reducing costs.
Results
Targeted anti-Aspergillus prophylaxis versus no anti-Aspergillus prophylaxis in individuals at high risk of invasive aspergillosis
Summary of Evidence
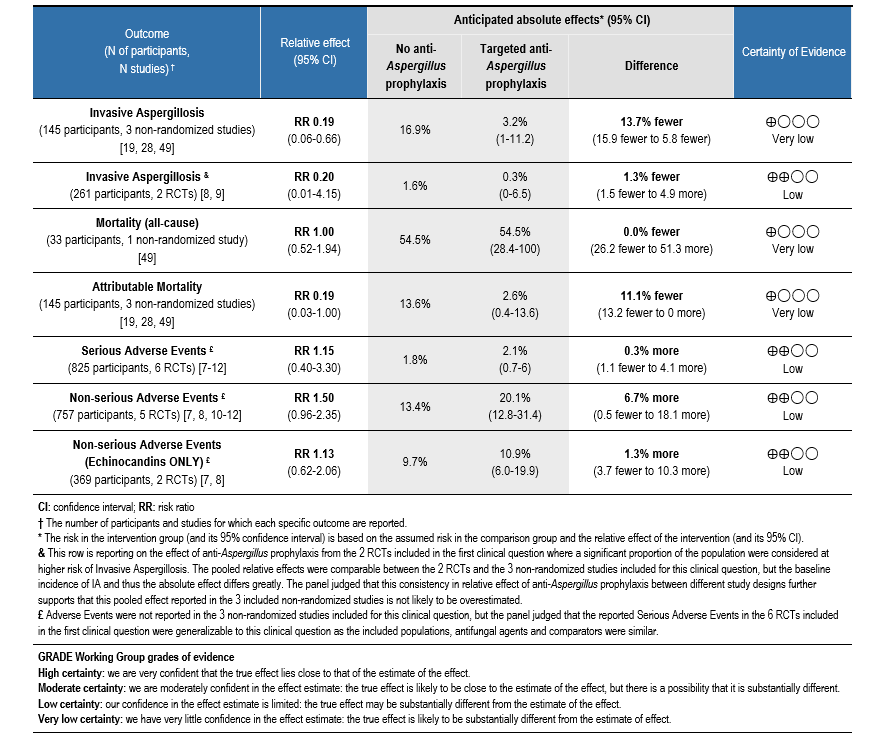
Our systematic review of the literature (spanning from 2000-2025) identified three non-randomized studies comparing the use of targeted anti-Aspergillus prophylaxis (either caspofungin, liposomal amphotericin B, and amphotericin B lipid complex) to not using anti-Aspergillus prophylaxis (no antifungal prophylaxis) in individuals at high risk of IA [19, 28, 49].
Table 3. Summary of Findings: Targeted Anti-Aspergillus Prophylaxis Versus No Anti-Aspergillus Prophylaxis in Liver Transplant Recipients
Rationale for Recommendation
When targeted prophylaxis was compared with no prophylaxis, the panel judged that the balance of benefits and harms favored targeted anti-Aspergillus prophylaxis in liver transplant recipients. Specifically, targeted prophylaxis is anticipated to provide a moderate reduction in IA incidence and IA attributable mortality, without evidence of excess harm compared to no prophylaxis although potential harms may vary depending on the antifungal class used. The panel agreed that the overall certainty of the evidence was very low due to risk of bias and imprecision related to small sample size and number of events.
The panel acknowledges that targeted anti-Aspergillus would increase direct costs related to drug acquisition, administration, and laboratory monitoring. Although cost-effectiveness could not be determined, the panel judged that the use of targeted anti-Aspergillus prophylaxis was acceptable for stakeholders. The panel assumed that patients would generally value an intervention that offers a favorable balance of benefits and harms. Because prophylaxis is usually provided in the inpatient setting for a limited duration, inequities are unlikely to be significant.
The guideline panel suggested using targeted anti-Aspergillus prophylaxis for liver transplant recipients considered at high risk of IA following transplantation (renal replacement therapy [RRT] in the peri-transplantation period, re-transplantation, or transplantation for fulminant hepatic failure), rather than no anti-Aspergillus prophylaxis.
Results
Targeted anti-aspergillus prophylaxis in individuals at high risk of invasive aspergillosis versus Universal anti-aspergillus prophylaxis
Summary of Evidence
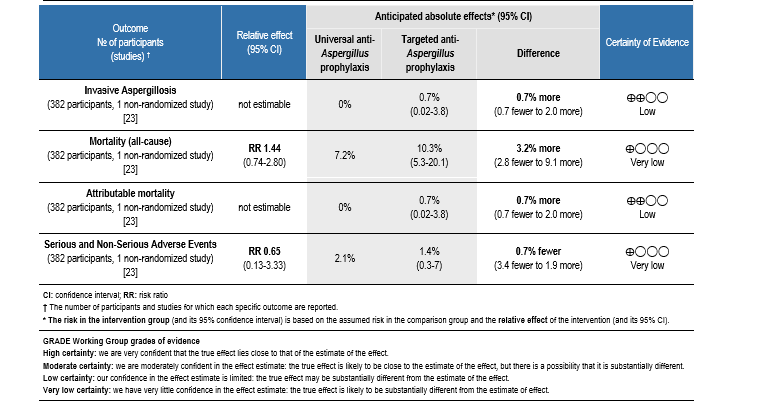
Our systematic review of the literature (spanning from 2000-2025) identified a single non-randomized retrospective study that directly compared targeted anti-Aspergillus prophylaxis with universal prophylaxis, in which both groups received voriconazole [23].
Table 4. Summary of Findings: Targeted Anti-Aspergillus Prophylaxis Versus Universal Anti-Aspergillus Prophylaxis in Liver Transplant Recipients
Rationale for Recommendation
The panel judged that the balance of benefits and harms does not clearly favor either strategy. Specifically, the evidence showed that targeted prophylaxis was anticipated to provide trivial undesirable effects (small to no increase in IA and attributable mortality) with trivial desirable effects (small to no reduction in adverse events [AEs]) as compared to universal prophylaxis. The panel agreed that the certainty in the evidence was very low due to the risk of bias associated with the study design as well as the imprecision.
The panel judged that restricting anti-Aspergillus prophylaxis to a targeted group of individuals was acceptable to stakeholders, largely because of stewardship benefits. The panel acknowledged that restricting anti-Aspergillus prophylaxis to target individuals at high risk of invasive disease would reduce drug-drug interactions, toxicities, and selective pressure for resistance, while also lowering direct drug acquisition and monitoring costs. Cost-effectiveness was not formally evaluated, but targeted prophylaxis was expected to be more resource-efficient than universal use. Patients are likely to value avoiding unnecessary antifungal exposure while still receiving protection when the risk is elevated. Restricting prophylaxis to high-risk groups was not expected to introduce inequity, as all patients meeting defined criteria would remain eligible. The panel also recognized that some centers may have local protocols for yeast prophylaxis that overlap with anti-Aspergillus prophylaxis, suggesting that the latter may not always represent a major incremental cost or use of additional resources. Overall, the panel assumed that most patients would support this targeted approach, though some variability in how stewardship considerations would be valued may exist.
The guideline panel suggested using targeted anti-Aspergillus prophylaxis in liver transplant recipients at high risk of IA following transplantation (RRT in the peri-transplantation period, re-transplantation, or transplantation for fulminant hepatic failure), rather than universal prophylaxis in all liver transplant recipients.
Clinical Question
In liver transplant recipients for whom anti-Aspergillus prophylaxis is indicated, what is the optimal choice of agent(s)?
Recommendation 3
In liver transplant recipients requiring anti-Aspergillus prophylaxis, we suggest using an echinocandin or a newer anti-mold triazole (voriconazole, posaconazole or isavuconazole) rather than amphotericin B formulations or itraconazole (conditional recommendation, very low certainty of evidence).
Remarks
- This recommendation prioritizes reducing adverse events (e.g., nephrotoxicity and hepatotoxicity), minimizing drug-drug interactions (especially with cyclosporine, tacrolimus, sirolimus and everolimus), and optimizing bioavailability.
- Among the anti-mold triazoles, the available evidence is derived primarily from studies evaluating voriconazole. To date, no peer-reviewed studies have specifically assessed posaconazole or isavuconazole for prophylaxis in liver transplant recipients. Based on indirect evidence from other transplant populations, these anti-mold triazoles (voriconazole, posaconazole and isavuconazole) are expected to provide comparable benefits.
Results
Summary of Evidence
Our systematic review of the literature (spanning from 2000-2025) identified two network meta-analysis reporting on the efficacy of universal antifungal prophylaxis for the prevention of invasive fungal infections (IFIs) [57, 58], although neither assessed differences in safety among antifungal agents. No RCTs comparing different antifungal agents used for targeted prophylaxis were identified. Our systematic review identified two non-randomized studies reporting on the use of either echinocandins or amphotericin B formulations as targeted prophylaxis in liver transplant recipients considered at high risk of IFIs [44, 59].
Rationale for Recommendation
When comparing anti-Aspergillus prophylaxis options in liver transplant recipients, the panel judged that the balance of benefits and harms generally favored echinocandins and the newer anti-mold triazoles (voriconazole, posaconazole and isavuconazole), primarily due to their more favorable side effect profile as compared to amphotericin B formulations (infusion-related reaction and nephrotoxicity) and itraconazole (gastrointestinal side effects and variable absorption). However, direct evidence in liver transplant recipients remains limited. To date, posaconazole has not been formally studied for prophylaxis in this population. Although isavuconazole use has been reported in a study that included liver transplant recipients, data specific to its effectiveness for prophylaxis have not yet been published. As a result, recommendations regarding posaconazole and isavuconazole are extrapolated from trial data in other transplant populations. Overall, the certainty in the evidence remains very low due to the paucity of head-to-head comparative studies and the small sample size of available cohort studies.
The panel judged that either voriconazole, posaconazole, isavuconazole or echinocandins are preferred for antifungal prophylaxis. Itraconazole is limited by unreliable absorption and significant drug-drug interactions. Voriconazole and posaconazole also have notable interactions, requiring careful monitoring. Amphotericin B formulations have limited tolerability at optimal dosing, are only available intravenously, and carry increased costs. Stewardship considerations may influence agent selection and differ across antifungal classes.
The guideline panel suggested using an echinocandin or a newer anti-mold triazole (voriconazole, posaconazole or isavuconazole) rather than amphotericin B formulations or itraconazole for targeted anti-Aspergillus prophylaxis for liver transplant recipients at high risk of IA in the post-transplantation period.
Kidney Transplant Recipients
Last Updated:
June 26, 2026Literature Review Conducted:
April 01, 2025This Recommendation Is Endorsed By The American Society of Transplantation (AST) and The Pediatric Infectious Diseases Society (PIDS)
Authors:
M. Hong Nguyen*, Jo-Anne H. Young*, Shahid Husain, Nitipong Permpalung, David R. Andes, Miranda So, Monica I. Ardura, Antonio C. Arrieta, Eric J. Bow, Pranatharthi H. Chandrasekar, Sharon C-A. Chen, Sarah P. Hammond, Sophia A. Koo, Thomas F. Patterson, George R. Thompson, Mindy G. Schuster**, C. Orla Morrissey**, Valéry Lavergne**Conclusion
Clinical Question
In kidney transplant recipients, what is the baseline risk of invasive aspergillosis in patients not receiving anti-Aspergillus prophylaxis and which factors increase this risk of IA?
Conclusion
Given the low pooled incidence of IA, the use of universal anti-Aspergillus prophylaxis is expected to provide limited benefits and thus a less favorable balance of benefits and harms. The current available evidence does not support the use of universal IA prophylaxis in kidney transplant recipients.
Results
Summary of Evidence
To understand the true burden of IA in kidney transplant recipients, a mapping review of the literature published from 2000 to 2025 was performed to determine the incidence of IA in kidney transplant recipients not receiving anti-Aspergillus prophylaxis [30, 34, 78-109]. Among 35,240 kidney transplant recipients from the 34 included observational studies, the pooled incidence of IA was 0.8% (95% CI 0.6 to 1.2%). The one-year all-cause mortality among 124 cases with available survival data was 45%. Two large United States database registry studies that used billing codes to detect cases of IA included a total of 90,608 patients [114, 115] and the pooled incidence for IA 0.4% (95% CI: 0.2% to 0.6%). Factors associated with increased IA risk included low volume transplant centers, older age, preceding bacterial pneumonia, Candida colonization (which may be a surrogate marker for severe immunosuppression), diabetes, chronic lung or heart disease, and leukopenia [80, 115]. Other factors that may increase risk include delayed graft function, acute rejection, and RRT [86, 89].
Pancreas Transplant Recipients
Last Updated:
June 26, 2026Literature Review Conducted:
April 01, 2025This Recommendation Is Endorsed By The American Society of Transplantation (AST) and The Pediatric Infectious Diseases Society (PIDS)
Authors:
M. Hong Nguyen*, Jo-Anne H. Young*, Shahid Husain, Nitipong Permpalung, David R. Andes, Miranda So, Monica I. Ardura, Antonio C. Arrieta, Eric J. Bow, Pranatharthi H. Chandrasekar, Sharon C-A. Chen, Sarah P. Hammond, Sophia A. Koo, Thomas F. Patterson, George R. Thompson, Mindy G. Schuster**, C. Orla Morrissey**, Valéry Lavergne**Conclusion
Clinical Question
In pancreas transplant recipients, what is the baseline risk of invasive aspergillosis in patients not receiving anti-Aspergillus prophylaxis and which factors increase this risk of IA?
Conlcusion
Given the low pooled incidence of IA, the use of universal anti-Aspergillus prophylaxis is expected to provide limited benefits and thus a less favorable balance of benefits and harms. The current available evidence does not support the use of universal IA prophylaxis in pancreas transplant recipients.
Results
Summary of Evidence
To understand the true burden of IA in pancreas transplant recipients, a mapping review of the literature published from 2000 to 2025 was performed to determine the incidence of IA in patients who did not receive anti-Aspergillus prophylaxis. Among 1,234 pancreas transplant recipients from 11 included observational studies [26, 87, 119-127], the pooled incidence of IA was 0.8% (95% CI 0.3% to 1.7%). The one-year all-cause mortality was 70%, although only three deaths were clearly attributable to IA. Although some reports suggest a higher incidence of IA among patients receiving lymphocyte-depleting agents such as alemtuzumab, available data are insufficient to confirm this association [120, 123, 125].
Lung Transplant Recipients
Last Updated:
June 26, 2026Literature Review Conducted:
April 01, 2025This Recommendation Is Endorsed By The American Society of Transplantation (AST) and The Pediatric Infectious Diseases Society (PIDS)
Authors:
Shahid Husain*, Nitipong Permpalung*, M. Hong Nguyen, Jo-Anne H. Young, Aadith Ashok, Miranda So, David R. Andes, Monica I. Ardura, Antonio C. Arrieta, Eric J. Bow, Pranatharthi H. Chandrasekar, Sharon C-A. Chen, Sarah P. Hammond, Sophia A. Koo, Thomas F. Patterson, George R. Thompson, C. Orla Morrissey**, Mindy G. Schuster**, Valéry Lavergne**Recommendations
Clinical Question
In lung transplant recipients, what is the optimal anti-Aspergillus prophylaxis strategy (universal prophylaxis, targeted prophylaxis, or preemptive therapy)?
Recommendation 1
In lung transplant recipients, we make no recommendation for or against universal anti-Aspergillus prophylaxis (no recommendation, knowledge gap).
Remarks
- The panel concluded that the potential benefits of the universal as compared to no anti-Aspergillus prophylaxis remain unclear. There are critical risks of bias in existing studies, unexplored sources of heterogeneity between studies, and serious concerns regarding their lack of generalizability to current clinical practice. Further studies are needed to evaluate the effectiveness and safety of antifungal agents particularly in respect to potential harms such as serious adverse events, drug-drug interactions, costs and challenges related to antimicrobial stewardship.
- The role of antifungal prophylaxis in lung transplantation remains complex due to the lack of high-quality evidence supporting a standardized approach, leading to significant variability in practice. Please refer to the “Considerations When Implementing a Prophylactic Strategy” section.
Recommendation 2
In lung transplant recipients, we make no recommendation for or against any targeted anti-Aspergillus prophylaxis or preemptive therapy rather than universal anti-Aspergillus prophylaxis (no recommendation, knowledge gap).
Remarks
- The panel concluded that the potential benefits of the different anti-Aspergillus prophylactic strategies (universal prophylaxis, targeted prophylaxis, and preemptive therapy) remain unclear. There are critical risks of bias in existing studies, unexplored sources of heterogeneity between studies, and serious concerns regarding their lack of generalizability to current clinical practice. Further studies are needed to evaluate the effectiveness and safety of antifungal agents in this setting, particularly in respect to potential harms such as serious adverse events, drug-drug interactions, costs and challenges related to antimicrobial stewardship.
- The role of antifungal prophylaxis in lung transplantation remains complex due to the lack of high-quality evidence supporting a standardized approach, leading to significant variability in practice. Please refer to the “Considerations When Implementing a Prophylactic Strategy” section.
Results
Universal anti-Aspergillus prophylaxis versus no anti-Aspergillus prophylaxis
Summary of Evidence
Our systematic review of the literature (spanning from 2000-2025) identified four observational studies [15-18] comparing universal anti-Aspergillus prophylaxis (utilizing either voriconazole or aerosolized amphotericin B with or without itraconazole) to the absence of anti-Aspergillus prophylaxis. Additionally, to better understand the true burden of IA in lung transplant recipients, a mapping review across 6 observational studies published from 2000 to 2025 was performed to determine the incidence of IA in lung transplant recipients not receiving anti-Aspergillus prophylaxis. [15-17, 21-23]
Table 5. Summary of Findings: Universal Anti-Aspergillus prophylaxis Versus No Anti-Aspergillus Prophylaxis in Lung Transplant Recipients
Limitations
The overall risk of bias of the identified evidence was judged to be critical, which precludes drawing meaningful conclusions. All three studies were single-center retrospective “before-and-after” cohort studies, a design inherently prone to biases. The inclusion of patients from older studies may compromise the validity of the conclusions, as evolving clinical practice, patient demographics, and healthcare standards could affect the findings’ generalizability to current clinical settings. Small sample sizes (55 to 274 patients) were prone to residual confounding and selection bias, undermining reliability. Moreover, the absence of critical baseline characteristics, such as Aspergillus colonization at transplant and use of anti-lymphocyte therapies, maintenance immunosuppressive regimens precluded meaningful comparisons. Similarly, Tofte 2012 noted significant mortality changes across two time periods, likely driven by shifts in clinical practices or inclusion of higher-risk patients rather than prophylaxis effects [15]. Additional limitations included the absence of surveillance bronchoscopies in two studies [16, 17], lack of therapeutic drug monitoring (TDM) for azoles in one study [15], and incomplete reporting on AE and adherence to the intended prophylaxis. Finally, the very high incidence of IA (>17%) in all four studies raises further concerns about their generalizability to current practice.
Our review revealed significant heterogeneity among the studies, but the small number of studies limited exploration of its sources. Potential contributors include differences in eras (patients enrolled in the 1990s vs later), population IA risk profiles, surveillance protocols (routine surveillance bronchoscopies and newer diagnostic tools), standards of care, prophylaxis types (agents, dosage, route of administration, and duration), or durations of follow-up. Without addressing these factors, the panel could not draw meaningful conclusions about the impact of antifungal prophylactic strategies on IA incidence. Consequently, the panel was unable to draw meaningful or definitive conclusions regarding the impact of antifungal prophylaxis on IA incidence.
Given the critical risk of bias, limited generalizability to current clinical practice, and unresolved sources of heterogeneity between studies, the panel concluded that the potential benefits of universal prophylaxis as compared to no anti-Aspergillus prophylaxis in lung transplant recipients remain uncertain.
Results
Universal anti-Aspergillus prophylaxis versus targeted anti-Aspergillus prophylaxis or pre-emptive therapy
Summary of Evidence
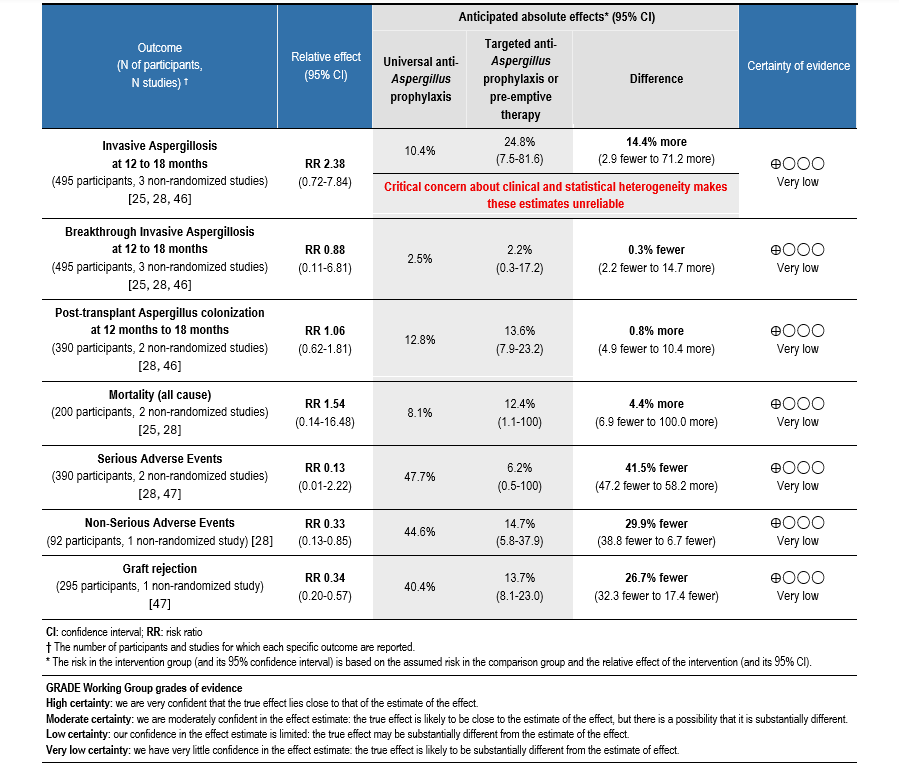
Our systematic review of the literature (spanning from 2000-2025) identified three observational studies reported across four publications [25, 28, 46, 47] that compared universal anti-Aspergillus prophylaxis with targeted anti-Aspergillus prophylaxis or preemptive therapy.
Table 6. Summary of Findings: Universal Anti-Aspergillus Prophylaxis Versus Targeted Anti-Aspergillus Prophylaxis or Preemptive Therapy in Lung Transplant Recipients
Limitations
The overall risk of bias of the identified evidence was judged to be critical, severely limiting the ability to draw meaningful conclusions. All three studies were single-center retrospective “before-and-after” cohort studies, each enrolling a relatively small number of participants. The most important methodological limitation across these studies was the simultaneous alterations of multiple variables, including the antifungal prophylactic strategy, the agent used, and the duration of prophylaxis. These concurrent changes precluded valid comparisons and attribution of outcomes to any one intervention component.
Additional limitations included: 1) the incomplete reporting on AE and adherence to the intended prophylaxis in two studies [25, 28] and significant non-adherence and interruption of prophylaxis in the universal prophylaxis group in Crone 2023 study [46, 47], 2) serious concerns about dose of itraconazole used in Linder 2021 study [25], 3) the lack of TDM for azoles in the three studies, and 4) missing data on pertinent baseline clinical characteristics in two studies [25, 28], precluded any meaningful comparison between the before-and-after periods.
Our review of the literature highlighted the large heterogeneity between the different studies identified. Sources of heterogeneity could not be explored due to the small number of studies identified, but may have been caused by a multitude of factors such as difference in eras (patients enrolled in the 2000s vs 2020s), included populations, baseline risk of IA, surveillance protocols (timing of surveillance newer diagnostic tools), standards of care, types of prophylaxis use (class of agents, dosage, route of administration, and duration), or durations of follow-up. Without further exploration of the potential sources of heterogeneity, the panel could not come to a meaningful conclusion on the potential effect of any type of antifungal prophylactic strategies on the incidence of IA.
Due to critical risk of bias of the studies identified and unexplorable sources of heterogeneity between studies, the panel concluded that no reliable inferences could be made regarding the relative effectiveness of the different prophylactic strategies and thus the potential benefits and harms of the different prophylactic strategies (universal or targeted prophylaxis) and preemptive therapy remain unknown.
Rationale for Recommendation
When comparing the different anti-Aspergillus prophylaxis strategies in lung transplant recipients, the panel judges that the balance of benefits and harms remains unknown. More specifically, potential benefits were not fully evaluable due to critical risk of bias (multiple study limitations), serious inconsistency (i.e. heterogeneity between studies), and indirectness (lack of generalizability).
Furthermore, potential harms are very heterogenous and agent-specific: 1) specific safety profile (toxicities, such as hepatotoxicity, bronchospasm), 2) specific drug interactions with immunosuppressive agents, 3) mode of administration, 4) availability of TDM, 5) total duration of prophylaxis (duration of immediate post-transplantation to life), 6) costs of agents and resources needed for administration, as well as 7) stewardship considerations. See the section on choice of agent(s) for more information.
The guideline panel makes no recommendation for or against anti-Aspergillus prophylactic strategies or for or against any specific anti-Aspergillus preemptive treatment strategies for lung transplant recipients in the post-transplantation period.
Considerations When Implementing a Prophylactic Strategy
The role of antifungal prophylaxis in lung transplantation remains complex due to the lack of high-quality evidence supporting a standardized approach, leading to significant variability in practice. Four main approaches—universal prophylaxis, targeted prophylaxis, preemptive therapy, and no prophylaxis and no preemptive therapy—are commonly employed, each with distinct advantages and limitations (See Table 7). Transplant centers must carefully balance clinical efficacy, toxicity, drug interactions, cost, and feasibility to determine the most practical prophylaxis strategy for use in their own center.
Table 7. Comparative Antifungal Prophylaxis Strategies in Lung Transplantation
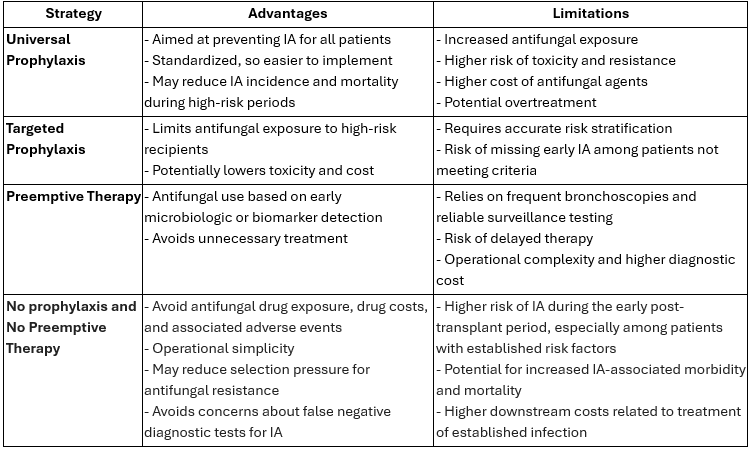
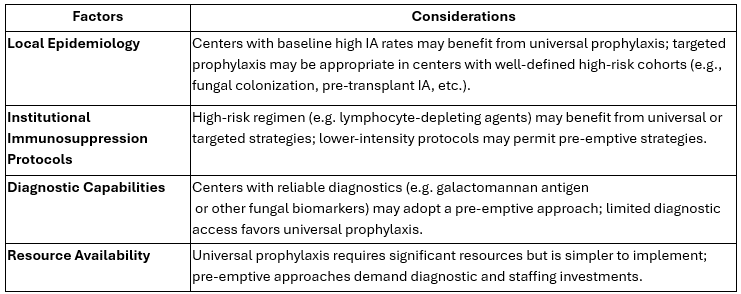
While Table 7 highlights the advantages and limitations of various antifungal prophylaxis strategies, it is important to emphasize that antifungal prophylaxis is not a one-size-fits-all approach. Instead, the choice should be tailored to transplant institutional factors, including local epidemiology, patient characteristics, immunosuppression protocols, diagnostic capabilities and available resources (See Table 8).
Table 8. Summary Table for Selecting Antifungal Prophylaxis Strategies
By carefully weighing these factors, transplant centers can design antifungal prophylaxis protocols that optimize patient outcomes while adapting to local conditions. If a prophylactic strategy is selected, continuous monitoring with regular assessment of IA rates, mortality, drug tolerability, and resistance patterns is essential. Stable IA infection rates and minimal toxicities support maintaining the current strategy. However, increases in breakthrough IA, toxicity, or resistance warrants a strategic evaluation and adjustment.
Clinical Question
In lung transplant recipients in whom anti-Aspergillus prophylaxis or preemptive therapy is considered, is there an optimal choice of antifungal agent(s)?
Recommendation 3
In lung transplant recipients in whom anti-Aspergillus prophylaxis or preemptive therapy is being considered, clinicians should select agent(s) based on the following factors: adverse events profile, drug-drug interactions, ease of administration and tolerability, associated costs and resources, availability, as well as local epidemiology (good practice statement).
Remarks
- In the absence of direct comparisons between different classes of agents in the reviewed evidence, the panel judged that an individualized approach for selecting anti-Aspergillus prophylaxis (if considered) is preferable.
- Comparison between triazoles is presented in the Table “Comparison of Characteristics, Tolerability and Cost of Anti-Mold Triazoles” and between different formulations of aerosolized amphotericin B in the Table “Comparison of Characteristics, Tolerability and Cost of Three Amphotericin B Formulations Adapted for Aerosolized Administration”.
Heart Transplant Recipients
Last Updated:
June 26, 2026Literature Review Conducted:
April 01, 2025This Recommendation Is Endorsed By The American Society of Transplantation (AST) and The Pediatric Infectious Diseases Society (PIDS)
Authors:
Shahid Husain*, Nitipong Permpalung*, M. Hong Nguyen, Jo-Anne H. Young, Aadith Ashok, Miranda So, David R. Andes, Monica I. Ardura, Antonio C. Arrieta, Eric J. Bow, Pranatharthi H. Chandrasekar, Sharon C-A. Chen, Sarah P. Hammond, Sophia A. Koo, Thomas F. Patterson, George R. Thompson, C. Orla Morrissey**, Mindy G. Schuster**, Valéry Lavergne**Conclusion
Clinical Question
In heart transplant recipients, what is the baseline risk of invasive aspergillosis in patients not receiving anti-Aspergillus prophylaxis and which factors increase this risk of IA?
Conclusion
Given the relatively low pooled incidence of IA, the use of universal anti-Aspergillus prophylaxis is likely to offer limited benefits and a less favorable balance of benefits and harms. The current evidence does not support routine universal prophylaxis against IA in heart transplant recipients.
Results
Summary of the Evidence
To understand the true burden of IA in heart transplant recipients, a mapping review of the literature published from 2000 to 2025 was performed to estimate the incidence of IA among patients who did not receive anti-Aspergillus prophylaxis. Among 6,005 heart transplant recipients from the 16 included studies [27, 79-93], the pooled incidence of IA was approximately 3.8% (95% CI 2.5 to 5.7%). Across the included studies, a range of patient-, procedure-, and environment-related factors were associated with the development of IA. The most consistently reported and reproducible risk factors were post-operative RRT, reoperation or redo thoracic surgery, cytomegalovirus infection, and augmented immunosuppression for treatment of rejection [83, 89, 92]. Additional factors reported in individual cohorts included prolonged mechanical ventilation or intubation, extracorporeal membrane oxygenation, hypoalbuminemia, multiple pre-transplant hospitalizations, prior Aspergillus colonization, and environmental or programmatic exposures such as hospital construction, ventilation system failures, or clustering of cases.
Appendix A: Pharmacology Tables
Last Updated:
June 26, 2026Literature Review Conducted:
April 01, 2025References and Notes
Background References
- Patterson TF, Thompson GR, 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis 2016; 63(4): e1–e60.
- Gras E, Azoyan L, Monzo-Gallo P, et al. Risk factors for invasive mould infections in adult patients with hematological malignancies and/or stem cell transplant: A systematic literature review and meta-analysis. J Infect 2025; 91(3): 106574.
- Thompson GR, 3rd, Young JH. Aspergillus Infections. N Engl J Med 2021; 385(16): 1496–509.
- Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis 2021; 21(6): e149–e62.
- Feys S, Lagrou K, Lauwers HM, et al. High Burden of COVID-19-Associated Pulmonary Aspergillosis in Severely Immunocompromised Patients Requiring Mechanical Ventilation. Clin Infect Dis 2024; 78(2): 361–70.
- Ghez D, Calleja A, Protin C, et al. Early-onset invasive aspergillosis and other fungal infections in patients treated with ibrutinib. Blood 2018; 131(17): 1955–9.
- Little JS, Aleissa MM, Beluch K, et al. Low incidence of invasive fungal disease following CD19 chimeric antigen receptor T-cell therapy for non-Hodgkin lymphoma. Blood Adv 2022; 6(16): 4821–30.
- Eades CP, Armstrong-James DPH. Invasive fungal infections in the immunocompromised host: Mechanistic insights in an era of changing immunotherapeutics. Med Mycol 2019; 57(Supplement_3): S307–S17.
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 2020; 71(6): 1367–76.
- Guo J, Xiao C, Tian W, et al. Performance of the Aspergillus galactomannan lateral flow assay with a digital reader for the diagnosis of invasive aspergillosis: a multicenter study. Eur J Clin Microbiol Infect Dis 2024; 43(2): 249–57.
- White PL, Bretagne S, Caliendo AM, et al. Aspergillus Polymerase Chain Reaction-An Update on Technical Recommendations, Clinical Applications, and Justification for Inclusion in the Second Revision of the EORTC/MSGERC Definitions of Invasive Fungal Disease. Clin Infect Dis 2021; 72(Suppl 2): S95–S101.
- Maertens JA, Thompson GR, 3rd, Spec A, et al. Olorofim for the treatment of invasive fungal diseases in patients with few or no therapeutic options: a single-arm, open-label, phase 2b study. Lancet Infect Dis 2025.
- Hodges MR, Tawadrous M, Cornely OA, et al. Fosmanogepix for the Treatment of Invasive Mold Diseases Caused by Aspergillus Species and Rare Molds: A Phase 2, Open-Label Study (AEGIS). Clin Infect Dis 2025.
- Pagano L, Maschmeyer G, Lamoth F, et al. Primary antifungal prophylaxis in hematological malignancies. Updated clinical practice guidelines by the European Conference on Infections in Leukemia (ECIL). Leukemia 2025; 39(7): 1547–57.
- Buil JB, Snelders E, Denardi LB, Melchers WJG, Verweij PE. Trends in Azole Resistance in Aspergillus fumigatus, the Netherlands, 1994-2016. Emerg Infect Dis 2019; 25(1): 176–8.
- Husain S, Mooney ML, Danziger-Isakov L, et al. A 2010 working formulation for the standardization of definitions of infections in cardiothoracic transplant recipients. J Heart Lung Transplant 2011; 30(4): 361–74.
- Husain S, Sole A, Alexander BD, et al. The 2015 International Society for Heart and Lung Transplantation Guidelines for the management of fungal infections in mechanical circulatory support and cardiothoracic organ transplant recipients: Executive summary. J Heart Lung Transplant 2016; 35(3): 261–82.
Methods References
- (IDSA) IDSoA. Handbook for Clinical Practice Guidelines Development. Available at: https://www.idsociety.org/globalassets/idsa/practice-guidelines/idsa-handbook-for-cpg-development-2020-01-09.pdf. Accessed September 15, 2025.
- Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011; 64(4): 383–94.
- Alonso-Coello P, Oxman AD, Moberg J, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ 2016; 353: i2089.
- Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. Clinical Practice Guidelines We Can Trust. In: Graham R, Mancher M, Wolman DM, Greenfield S, Steinberg E. Washington, DC: National Academies Press (US), 2011.
- Ascioglu S, Rex JH, de Pauw B, et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis 2002; 34(1): 7–14.
- De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 2008; 46(12): 1813–21.
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 2020; 71(6): 1367–76.
- Husain S, Mooney ML, Danziger-Isakov L, et al. A 2010 working formulation for the standardization of definitions of infections in cardiothoracic transplant recipients. J Heart Lung Transplant 2011; 30(4): 361–74.
- Segal BH, Herbrecht R, Stevens DA, et al. Defining responses to therapy and study outcomes in clinical trials of invasive fungal diseases: Mycoses Study Group and European Organization for Research and Treatment of Cancer consensus criteria. Clin Infect Dis 2008; 47(5): 674–83.
- Marinelli T, Davoudi S, Foroutan F, Orchanian-Cheff A, Husain S. Antifungal prophylaxis in adult lung transplant recipients: Uncertainty despite 30 years of experience. A systematic review of the literature and network meta-analysis. Transpl Infect Dis 2022; 24(3): e13832.
- Covidence. Covidence Systematic Review Software VHI, Melbourne, Australia. Available at: www.covidence.org. Accessed September 15, 2025.
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327(7414): 557–60.
- Ioannidis JP, Trikalinos TA. The appropriateness of asymmetry tests for publication bias in meta-analyses: a large survey. CMAJ 2007; 176(8): 1091–6.
- The Cochrane Collaboration. RevMan: Systematic review and meta-analysis tool for researchers worldwide. Available at: https://revman.cochrane.org/info. Accessed Septmeber 15, 2025.
- Sterne JA, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016; 355: i4919.
- Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med 2013; 158(4): 280–6.
- GRADE. GRADE Book. Available at: https://book.gradepro.org. Accessed September 15, 2025.
- GRADE. GRADEpro GDT: GRADEpro Guideline Development Tool. Available at: https://www.gradepro.org/. Accessed September 15, 2025.
- Andrews JC, Schunemann HJ, Oxman AD, et al. GRADE guidelines: 15. Going from evidence to recommendation-determinants of a recommendation's direction and strength. J Clin Epidemiol 2013; 66(7): 726–35.
- Guyatt GH, Alonso-Coello P, Schunemann HJ, et al. Guideline panels should seldom make good practice statements: guidance from the GRADE Working Group. J Clin Epidemiol 2016; 80: 3–7.
Liver, Kidney, and Pancreas References
- Husain S, Tollemar J, Dominguez EA, et al. Changes in the spectrum and risk factors for invasive candidiasis in liver transplant recipients: prospective, multicenter, case-controlled study. Transplantation 2003; 75(12): 2023-9.
- Neofytos D, Fishman JA, Horn D, et al. Epidemiology and outcome of invasive fungal infections in solid organ transplant recipients. Transpl Infect Dis 2010; 12(3): 220-9.
- Eschenauer GA, Lam SW, Carver PL. Antifungal prophylaxis in liver transplant recipients. Liver Transpl 2009; 15(8): 842-58.
- Barchiesi F, Mazzocato S, Mazzanti S, et al. Invasive aspergillosis in liver transplant recipients: epidemiology, clinical characteristics, treatment, and outcomes in 116 cases. Liver Transpl 2015; 21(2): 204-12.
- Salmanton-Garcia J, Giacinta A, Giannella M, et al. Current trends on antifungal prophylaxis in solid organ transplantation: a study from ESCMID-EFISG, ESCMID-ESGICH, SITA, and SEIMC-GESITRA-IC. Infection 2025.
- Singh N, Wagener MM, Cacciarelli TV, Levitsky J. Antifungal management practices in liver transplant recipients. Am J Transplant 2008; 8(2): 426-31.
- Kang W-H, Song G-W, Lee S-G, et al. A Multicenter, Randomized, Open-Label Study to Compare Micafungin with Fluconazole in the Prophylaxis of Invasive Fungal Infections in Living-Donor Liver Transplant Recipients. Journal of Gastrointestinal Surgery 2020; 24(4): 832-40.
- Winston DJ, Limaye AP, Pelletier S, et al. Randomized, double-blind trial of anidulafungin versus fluconazole for prophylaxis of invasive fungal infections in high-risk liver transplant recipients. Am J Transplant 2014; 14(12): 2758-64.
- Hadley S, Huckabee C, Pappas PG, et al. Outcomes of antifungal prophylaxis in high-risk liver transplant recipients. Transpl Infect Dis 2009; 11(1): 40-8.
- Sharpe MD, Ghent C, Grant D, Horbay GL, McDougal J, David Colby W. Efficacy and safety of itraconazole prophylaxis for fungal infections after orthotopic liver transplantation: a prospective, randomized, double-blind study. Transplantation 2003; 76(6): 977-83.
- Biancofiore G, Bindi ML, Baldassarri R, et al. Antifungal prophylaxis in liver transplant recipients: a randomized placebo-controlled study. Transpl Int 2002; 15(7): 341-7.
- Winston DJ, Busuttil RW. Randomized controlled trial of oral itraconazole solution versus intravenous/oral fluconazole for prevention of fungal infections in liver transplant recipients. Transplantation 2002; 74(5): 688-95.
- De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 2008; 46(12): 1813-21.
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 2020; 71(6): 1367-76.
- Aliakbarian M, Khodashahi R, Rezayat KA, et al. Manifestations, prevalence, management and outcome of Invasive Aspergillosis in Post-Liver Transplant Patients. Curr Drug Saf 2022.
- Badiee P, Alborzi A, Malekhosseini SA, Nikeghbalian S, Shakiba E. Determining the incidence of aspergillosis after liver transplant. Exp Clin Transplant 2010; 8(3): 220-3.
- Balogh J, Gordon Burroughs S, Boktour M, et al. Efficacy and cost-effectiveness of voriconazole prophylaxis for prevention of invasive aspergillosis in high-risk liver transplant recipients. Liver Transpl 2016; 22(2): 163-70.
- Boutin C-A, Durocher F, Beauchemin S, Ziegler D, Abou Chakra CN, Dufresne SF. Breakthrough Invasive Fungal Infections in Patients With High-Risk Hematological Disorders Receiving Voriconazole and Posaconazole Prophylaxis: A Systematic Review. Clinical Infectious Diseases 2024; 79(1): 151-60.
- Chakravarti A, Butler-Laporte G, Carrier FM, et al. Targeted caspofungin prophylaxis for invasive aspergillosis in high-risk liver transplant recipients, a single-center experience. Transplant Infectious Disease 2021; 23(4).
- Chen YC, Huang TS, Wang YC, et al. Effect of Prophylactic Antifungal Protocols on the Prognosis of Liver Transplantation: A Propensity Score Matching and Multistate Model Approach. Biomed Res Int 2016; 2016: 6212503.
- Duchini A, Redfield DC, McHutchison JG, Brunson ME, Pockros PJ. Aspergillosis in liver transplant recipients: successful treatment and improved survival using a multistep approach. South Med J 2002; 95(8): 897-9.
- Ebrahimi A, Dashti H, Mohammadpour Z, Ahmadinejad Z. Invasive Fungal Infections With Good Survival Following Liver Transplant: A Single-Center Experience From a Developing Country. Exp Clin Transplant 2020; 18(2): 196-200.
- Eschenauer GA, Kwak EJ, Humar A, et al. Targeted versus universal antifungal prophylaxis among liver transplant recipients. American Journal of Transplantation 2015; 15(1): 180-9.
- Fortún J, Martín-Davila P, Moreno S, et al. Prevention of invasive fungal infections in liver transplant recipients: the role of prophylaxis with lipid formulations of amphotericin B in high-risk patients. J Antimicrob Chemother 2003; 52(5): 813-9.
- Fortún J, Muriel A, Martín-Dávila P, et al. Caspofungin versus fluconazole as prophylaxis of invasive fungal infection in high-risk liver transplantation recipients: A propensity score analysis. Liver Transpl 2016; 22(4): 427-35.
- Gavalda J, Len O, San Juan R, et al. Risk factors for invasive aspergillosis in solid-organ transplantrecipients: a case-control study. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 2005; 41(1): 52-9.
- Giannella M, Bartoletti M, Morelli M, et al. Antifungal prophylaxis in liver transplant recipients: one size does not fit all. Transpl Infect Dis 2016; 18(4): 538-44.
- Hellinger WC, Bonatti H, Yao JD, et al. Risk stratification and targeted antifungal prophylaxis for prevention of aspergillosis and other invasive mold infections after liver transplantation. Liver Transplantation 2005; 11(6): 656-62.
- Jorgenson MR, Descourouez JL, Marka NA, et al. A targeted fungal prophylaxis protocol with static dosed fluconazole significantly reduces invasive fungal infection after liver transplantation. Transpl Infect Dis 2019; 21(5): e13156.
- Ju MK, Joo DJ, Kim SJ, et al. Invasive pulmonary aspergillosis after solid organ transplantation: diagnosis and treatment based on 28 years of transplantation experience. Transplant Proc 2009; 41(1): 375-8.
- Ok Atılgan A, Özdemir BH, Kırnap M, et al. Invasive fungal infections in liver transplant recipients. Exp Clin Transplant 2014; 12 Suppl 1: 110-6.
- Karadag HI, Andacoglu O, Papadakis M, Paul A, Oezcelik A, Malamutmann E. Invasive Fungal Infections After Liver Transplantation: A Retrospective Matched Controlled Risk Analysis. Ann Transplant 2021; 26: e930117.
- Lavezzo B, Patrono D, Tandoi F, et al. A simplified regimen of targeted antifungal prophylaxis in liver transplant recipients: A single-center experience. Transpl Infect Dis 2018; 20(2): e12859.
- Morgan J, Wannemuehler KA, Marr KA, et al. Incidence of invasive aspergillosis following hematopoietic stem cell and solid organ transplantation: interim results of a prospective multicenter surveillance program. Med Mycol 2005; 43 Suppl 1: S49-58.
- Nagao M, Fujimoto Y, Yamamoto M, et al. Epidemiology of invasive fungal infections after liver transplantation and the risk factors of late-onset invasive aspergillosis. J Infect Chemother 2016; 22(2): 84-9.
- Neyra KM, Brizendine KD. Retrospective study evaluating the performance of risk factors for invasive mold infections in liver transplantation. Transpl Infect Dis 2020; 22(1): e13223.
- Ohkubo T, Sugawara Y, Takayama T, Kokudo N, Makuuchi M. The risk factors of fungal infection in living-donor liver transplantations. J Hepatobiliary Pancreat Sci 2012; 19(4): 382-8.
- Pacholczyk M, Lagiewska B, Lisik W, Wasiak D, Chmura A. Invasive fungal infections following liver transplantation - risk factors, incidence and outcome. Ann Transplant 2011; 16(3): 14-6.
- Pappas PG, Andes D, Schuster M, et al. Invasive fungal infections in low-risk liver transplant recipients: a multi-center prospective observational study. Am J Transplant 2006; 6(2): 386-91.
- Perrella A, Esposito C, Pisaniello D, et al. Role of liposomal amphotericin B prophylaxis after liver transplantation compared with fluconazole for high-risk patients. impact on infections and mortality within one year. Transplant Proc 2012; 44(7): 1977-81.
- Rabkin JM, Oroloff SL, Corless CL, et al. Association of fungal infection and increased mortality in liver transplant recipients. Am J Surg 2000; 179(5): 426-30.
- Raghuram A, Restrepo A, Safadjou S, et al. Invasive fungal infections following liver transplantation: incidence, risk factors, survival, and impact of fluconazole-resistant Candida parapsilosis (2003-2007). Liver Transpl 2012; 18(9): 1100-9.
- Reed A, Herndon JB, Ersoz N, et al. Effect of prophylaxis on fungal infection and costs for high-risk liver transplant recipients. Liver Transpl 2007; 13(12): 1743-50.
- Rinaldi M, Bartoletti M, Ferrarese A, et al. Breakthrough invasive fungal infection after liver transplantation in patients on targeted antifungal prophylaxis: A prospective multicentre study. Transplant Infectious Disease 2021; 23(4).
- Saliba F, Delvart V, Ichaï P, et al. Fungal infections after liver transplantation: outcomes and risk factors revisited in the MELD era. Clin Transplant 2013; 27(4): E454-61.
- San-Juan R, Aguado JM, Lumbreras C, et al. Universal prophylaxis with fluconazole for the prevention of early invasive fungal infection in low-risk liver transplant recipients. Transplantation 2011; 92(3): 346-50.
- Sganga G, Bianco G, Frongillo F, Lirosi MC, Nure E, Agnes S. Fungal infections after liver transplantation: incidence and outcome. Transplant Proc 2014; 46(7): 2314-8.
- Shi SH, Lu AW, Shen Y, et al. Spectrum and risk factors for invasive candidiasis and non-Candida fungal infections after liver transplantation. Chin Med J (Engl) 2008; 121(7): 625-30.
- Singh N, Paterson DL, Gayowski T, Wagener MM, Marino IR. Preemptive prophylaxis with a lipid preparation of amphotericin B for invasive fungal infections in liver transplant recipients requiring renal replacement therapy. Transplantation 2001; 71(7): 910-3.
- Trudeau RE, Bowman LJ, Wills AR, Crippin JS, Chapman WC, Anderson C. Once weekly fluconazole for antifungal prophylaxis post-liver transplantation. HPB (Oxford) 2013; 15(7): 541-7.
- Zhou T, Xue F, Han LZ, et al. Invasive fungal infection after liver transplantation: risk factors and significance of immune cell function monitoring. J Dig Dis 2011; 12(6): 467-75.
- Zicker M, Colombo AL, Ferraz-Neto BH, Camargo LF. Epidemiology of fungal infections in liver transplant recipients: a six-year study of a large Brazilian liver transplantation centre. Mem Inst Oswaldo Cruz 2011; 106(3): 339-45.
- Fortun J, Martin-Davila P, Moreno S, et al. Prevention of invasive fungal infections in liver transplant recipients: the role of prophylaxis with lipid formulations of amphotericin B in high-risk patients. J Antimicrob Chemother 2003; 52(5): 813-9.
- Ascioglu S, Rex JH, de Pauw B, et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis 2002; 34(1): 7-14.
- Phoompoung P, Herrera S, Perez Cortes Villalobos A, Foroutan F, Orchanian-Cheff A, Husain S. Risk factors of invasive fungal infections in liver transplant recipients: A systematic review and meta-analysis. Am J Transplant 2022; 22(4): 1213-29.
- Kimura M, Rinaldi M, Kothari S, et al. Invasive aspergillosis in liver transplant recipients in the current era. Am J Transplant 2024; 24(11): 2092-107.
- Evans JD, Morris PJ, Knight SR. Antifungal prophylaxis in liver transplantation: a systematic review and network meta-analysis. Am J Transplant 2014; 14(12): 2765-76.
- Liu Y, Lan C, Qin S, et al. Efficacy of anti-fungal agents for invasive fungal infection prophylaxis in liver transplant recipients: A network meta-analysis. Mycoses 2022; 65(10): 906-17.
- Sun HY, Cacciarelli TV, Singh N. Micafungin versus amphotericin b lipid complex for the prevention of invasive fungal infections in high-risk liver transplant recipients. Transplantation 2013; 96(6): 573-8.
- Doria C, Bodzin AS, Vaccino S, Daskalakis C, Krawitz S, Ramirez CB. A retrospective analysis of the use of caspofungin in recipients of liver transplant with a modified high index of suspicion for fungal infection. A critical review of mortality, acute cellular rejection, infections, and changes in the liver function tests while on caspofungin. Clin Transplant 2011; 25(4): 569-75.
- Fortun J, Martin-Davila P, Montejo M, et al. Prophylaxis with caspofungin for invasive fungal infections in high-risk liver transplant recipients. Transplantation 2009; 87(3): 424-35.
- Perrella A, Esposito C, Amato G, et al. Antifungal prophylaxis with liposomal amphotericin B and caspofungin in high-risk patients after liver transplantation: impact on fungal infections and immune system. Infect Dis (Lond) 2016; 48(2): 161-6.
- Breitkopf R, Treml B, Senoner T, Bukumiric Z, Rajsic S. Invasive Fungal Breakthrough Infections under Targeted Echinocandin Prophylaxis in High-Risk Liver Transplant Recipients. J Fungi (Basel) 2023; 9(2).
- Saliba F, Pascher A, Cointault O, et al. Randomized trial of micafungin for the prevention of invasive fungal infection in high-risk liver transplant recipients. Clin Infect Dis 2015; 60(7): 997-1006.
- Sun HY, Cacciarelli TV, Singh N. Micafungin versus amphotericin B lipid complex for the prevention of invasive fungal infections in high-risk liver transplant recipients. Transplantation 2013; 96(6): 573-8.
- Jimenez-Ortigosa C, Moore C, Denning DW, Perlin DS. Emergence of Echinocandin Resistance Due to a Point Mutation in the fks1 Gene of Aspergillus fumigatus in a Patient with Chronic Pulmonary Aspergillosis. Antimicrob Agents Chemother 2017; 61(12).
- Marini R. Breakthrough Fungal Infections in Solid Organ Transplant (SOT) Recipients Receiving Prophylaxis with Isavuconazole and Other Antifungal Agents Liver Transplant Recipients. 3rd ASM Microbe. Atlanta, GA, United States, 2018.
- D'Arcy ME, Pfeiffer RM, Rivera DR, et al. Voriconazole and the Risk of Keratinocyte Carcinomas Among Lung Transplant Recipients in the United States. JAMA Dermatol 2020; 156(7): 772-9.
- Meis JF, Chowdhary A, Rhodes JL, Fisher MC, Verweij PE. Clinical implications of globally emerging azole resistance in Aspergillus fumigatus. Philos Trans R Soc Lond B Biol Sci 2016; 371(1709).
- Castroagudin JF, Ponton C, Bustamante M, et al. Prospective interventional study to evaluate the efficacy and safety of liposomal amphotericin B as prophylaxis of fungal infections in high-risk liver transplant recipients. Transplant Proc 2005; 37(9): 3965-7.
- Tollemar J, Hockerstedt K, Ericzon BG, Jalanko H, Ringden O. Liposomal amphotericin B prevents invasive fungal infections in liver transplant recipients. A randomized, placebo-controlled study. Transplantation 1995; 59(1): 45-50.
- Lorf T, Braun F, Ruchel R, Muller A, Sattler B, Ringe B. Systemic mycoses during prophylactical use of liposomal amphotericin B (Ambisome) after liver transplantation. Mycoses 1999; 42(1-2): 47-53.
- Antunes AM, Teixeira C, Corvo ML, Perdigoto R, Barroso E, Marcelino P. Prophylactic use of liposomal amphotericin B in preventing fungal infections early after liver transplantation: a retrospective, single-center study. Transplant Proc 2014; 46(10): 3554-9.
- Perlin DS, Rautemaa-Richardson R, Alastruey-Izquierdo A. The global problem of antifungal resistance: prevalence, mechanisms, and management. Lancet Infect Dis 2017; 17(12): e383-e92.
- Botero Aguirre JP, Restrepo Hamid AM. Amphotericin B deoxycholate versus liposomal amphotericin B: effects on kidney function. Cochrane Database Syst Rev 2015; 2015(11): CD010481.
- Heylen L, Maertens J, Naesens M, et al. Invasive aspergillosis after kidney transplant: case-control study. Clin Infect Dis 2015; 60(10): 1505-11.
- Sigera LSM, Denning DW. Invasive Aspergillosis after Renal Transplantation. J Fungi (Basel) 2023; 9(2).
- Ezzatzadegan S, Chen S, Chapman JR. Invasive fungal infections after renal transplantation. Int J Organ Transplant Med 2012; 3(1): 18-25.
- Boan P, Swaminathan R, Irish A. Infectious complications in indigenous renal transplant recipients in Western Australia. Intern Med J 2017; 47(6): 648-55.
- Hoyo I, Sanclemente G, de la Bellacasa JP, et al. Epidemiology, clinical characteristics, and outcome of invasive aspergillosis in renal transplant patients. Transpl Infect Dis 2014; 16(6): 951-7.
- Pérez-Sáez MJ, Mir M, Montero MM, et al. Invasive aspergillosis in kidney transplant recipients: a cohort study. Exp Clin Transplant 2014; 12(2): 101-5.
- Santos T, Aguiar B, Santos L, et al. Invasive Fungal Infections After Kidney Transplantation: A Single-center Experience. Transplant Proc 2015; 47(4): 971-5.
- Sahin SZ, Akalin H, Ersoy A, et al. Invasive Fungal Infections in Renal Transplant Recipients: Epidemiology and Risk Factors. Mycopathologia 2015; 180(1-2): 43-50.
- Balcan B, Ozcelik U, Ugurlu AO, Aydin M, Nalcaci S, Yarbug Karakayali F. Increased Mortality Among Renal Transplant Patients With Invasive Pulmonary Aspergillus Infection. Prog Transplant 2018; 28(4): 349-53.
- Guimarães LF, Halpern M, de Lemos AS, et al. Invasive Fungal Disease in Renal Transplant Recipients at a Brazilian Center: Local Epidemiology Matters.Transplant Proc 2016; 48(7): 2306-9.
- Seok H, Huh K, Cho SY, et al. Risk factors for development and mortality of invasive pulmonary Aspergillosis in kidney transplantation recipients. Eur J Clin Microbiol Infect Dis 2020; 39(8): 1543-50.
- van Delden C, Stampf S, Hirsch HH, et al. Burden and Timeline of Infectious Diseases in the First Year After Solid Organ Transplantation in the Swiss Transplant Cohort Study. Clin Infect Dis 2020; 71(7): e159-e69.
- Sommerer C, Schröter I, Gruneberg K, et al. Incidences of Infectious Events in a Renal Transplant Cohort of the German Center of Infectious Diseases (DZIF). Open Forum Infect Dis 2022; 9(7): ofac243.
- Zou J, Jin Z. Clinical characteristics and outcomes of invasive pulmonary aspergillosis in renal transplant recipients: A single-center experience. Transpl Immunol 2025; 88: 102150.
- Cornet M, Fleury L, Maslo C, Bernard JF, Brücker G. Epidemiology of invasive aspergillosis in France: a six-year multicentric survey in the Greater Paris area. J Hosp Infect 2002; 51(4): 288-96.
- Parajuli S, Wick A, Pandeya S, et al. The feared five fungal infections in kidney transplant recipients: A single-center 20-year experience. Clin Transplant 2018; 32(7): e13289.
- Badiee P, Kordbacheh P, Alborzi A, Zeini F, Mirhendy H, Mahmoody M. Fungal infections in solid organ recipients. Exp Clin Transplant 2005; 3(2): 385-9.
- Einollahi B, Lessan-Pezeshki M, Pourfarziani V, et al. Invasive fungal infections following renal transplantation: a review of 2410 recipients. Ann Transplant 2008; 13(4): 55-8.
- Cole E, Landsberg D, Russell D, et al. A pilot study of steroid-free immunosuppression in the prevention of acute rejection in renal allograft recipients. Transplantation 2001; 72(5): 845-50.
- Rao KH, Jha R, Narayan G, Sinha S. Opportunistic infections following renal transplantation. Indian J Med Microbiol 2002; 20(1): 47-9.
- Tharayil John G, Shankar V, Talaulikar G, et al. Epidemiology of systemic mycoses among renal-transplant recipients in India. Transplantation 2003; 75(9): 1544-51.
- Agrawal V, Gupta RK, Jain M. Invasive fungal infections in renal allograft recipients. Indian J Pathol Microbiol 2005; 48(4): 448-52.
- Patel MH, Patel RD, Vanikar AV, et al. Invasive fungal infections in renal transplant patients: a single center study. Ren Fail 2017; 39(1): 294-8.
- Shekar M, Elumalai R, Elayaperumal I, et al. Prevalence and outcome of systemic fungal infections in renal transplant recipients - A tertiary care experience. Saudi J Kidney Dis Transpl 2019; 30(5): 1137-43.
- Gupta KL, Bagai S, Ramachandran R, et al. Fungal infection in post-renal transplant patient: Single-center experience. Indian J Pathol Microbiol 2020; 63(4): 587-92.
- Murty M, Saxena VK, Sharma UK, Tandon S, Sharma P. Renal Transplantation: Experience at a Single Centre. Med J Armed Forces India 2009; 65(1): 18-22.
- Jain S, Bhadauria D, Prasad R, et al. Aetiology, management, and outcome of lower respiratory tract infection in renal allograft recipients - A report from a tropical country. Lung India 2022; 39(6): 545-52.
- Veroux M, Corona D, Gagliano M, et al. Voriconazole in the treatment of invasive aspergillosis in kidney transplant recipients. Transplant Proc 2007; 39(6): 1838-40.
- Sharifipour F, Rezaeetalab F, Naghibi M. Pulmonary fungal infections in kidney transplant recipients: an 8-year study. Transplant Proc 2009; 41(5): 1654-6.
- Thielke JJ, West-Thielke PM, Herren HL, et al. Living donor kidney transplantation across positive crossmatch: the University of Illinois at Chicago experience. Transplantation 2009; 87(2): 268-73.
- Trabelsi H, Néji S, Sellami H, et al. Invasive fungal infections in renal transplant recipients: about 11 cases. J Mycol Med 2013; 23(4): 255-60.
- Chayakulkeeree M, Vongwiwatana A. Invasive mold infection in kidney transplant recipients: observation of early-onset mucormycosis. Transplant Proc 2014; 46(2): 595-7.
- Vathsala A, Ona ET, Tan SY, et al. Randomized trial of Alemtuzumab for prevention of graft rejection and preservation of renal function after kidney transplantation. Transplantation 2005; 80(6): 765-74.
- Alangaden GJ, Thyagarajan R, Gruber SA, et al. Infectious complications after kidney transplantation: current epidemiology and associated risk factors. Clin Transplant 2006; 20(4): 401-9.
- Segal BH, Herbrecht R, Stevens DA, et al. Defining responses to therapy and study outcomes in clinical trials of invasive fungal diseases: Mycoses Study Group and European Organization for Research and Treatment of Cancer consensus criteria. Clin Infect Dis 2008; 47(5): 674-83.
- Altiparmak MR, Apaydin S, Trablus S, et al. Systemic fungal infections after renal transplantation. Scand J Infect Dis 2002; 34(4): 284-8.
- Castaldo P, Stratta RJ, Wood RP, et al. Clinical spectrum of fungal infections after orthotopic liver transplantation. Arch Surg 1991; 126(2): 149-56.
- Horvath JA, Dummer S. The use of respiratory-tract cultures in the diagnosis of invasive pulmonary aspergillosis. Am J Med 1996; 100(2): 171-8.
- Abbott KC, Hypolite I, Poropatich RK, et al. Hospitalizations for fungal infections after renal transplantation in the United States. Transpl Infect Dis 2001; 3(4): 203-11.
- Leitheiser S, Harner A, Waller JL, et al. Risk Factors Associated With Invasive Fungal Infections in Kidney Transplant Patients. Am J Med Sci 2020; 359(2): 108-16.
- Sever MS, Kazancioğlu R, Yildiz A, et al. Outcome of living unrelated (commercial) renal transplantation. Kidney Int 2001; 60(4): 1477-83.
- Kennedy SE, Shen Y, Charlesworth JA, et al. Outcome of overseas commercial kidney transplantation: an Australian perspective. Med J Aust 2005; 182(5): 224-7.
- Al Salmi I, Metry AM, Al Ismaili F, et al. Transplant tourism and invasive fungal infection. Int J Infect Dis 2018; 69: 120-9.
- López-Medrano F, Muñoz de la Espada M, Pérez-Jacoiste Asín MA, et al. Fluconazole versus micafungin for initial antifungal prophylaxis against Candida in pancreas transplant recipients: A comparative study of two consecutive periods. Mycoses 2022; 65(5): 517-25.
- Zachary J, Chen JM, Sharfuddin A, et al. Epidemiology and Risk Factors for Invasive Fungal Infections in Pancreas Transplant in the Absence of Postoperative Antifungal Prophylaxis. Open Forum Infect Dis 2023; 10(11): ofad478.
- Knight RJ, Kerman RH, Zela S, et al. Thymoglobulin, sirolimus, and reduced-dose cyclosporine provides excellent rejection prophylaxis for pancreas transplantation. Transplantation 2003; 75(8): 1301-6.
- Michalak G, Kwiatkowski A, Bieniasz M, et al. Infectious complications after simultaneous pancreas-kidney transplantation. Transplant Proc 2005; 37(8): 3560-3.
- Nath DS, Kandaswamy R, Gruessner R, Sutherland DE, Dunn DL, Humar A. Fungal infections in transplant recipients receiving alemtuzumab. Transplant Proc 2005; 37(2): 934-6.
- Nikeghbalian S, Malek-Hosseini SA, Salahi H, et al. Pancreas transplantation in shiraz organ transplant center; the first Iranian experience. Arch Iran Med 2008; 11(5): 490-6.
- Berger N, Wirmsberger R, Kafka R, et al. Infectious complications following 72 consecutive enteric-drained pancreas transplants. Transpl Int 2006; 19(7): 549-57.
- Fontana I, Bertocchi M, Diviacco P, et al. Infections after simultaneous pancreas and kidney transplantation: a single-center experience. Transplant Proc 2009; 41(4): 1333-5.
- Shaikh SA, Zimmerman A, Nolan A, Cooper M, Abrams PL. The incidence of fungal infections in pancreas transplant recipients in the absence of systemic antifungal prophylaxis. Clin Transplant 2019; 33(10): e13691.
Lung and Heart References
- Christie JD, Van Raemdonck D, Fisher AJ. Lung Transplantation. N Engl J Med 2024; 391(19): 1822–36.
- Courtwright AM, Doyon JB, Blumberg EA, et al. Infectious complications associated with bronchial anastomotic dehiscence in lung transplant recipients. Clin Transplant 2023; 37(10): e15040.
- Hsu JL, Khan MA, Sobel RA, et al. Aspergillus fumigatus invasion increases with progressive airway ischemia. PLoS One 2013; 8(10): e77136.
- Samanta P, Clancy CJ, Marini RV, et al. Isavuconazole Is as Effective as and Better Tolerated Than Voriconazole for Antifungal Prophylaxis in Lung Transplant Recipients. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2021; 73(3): 416–26.
- Cahill BC, Hibbs JR, Savik K, et al. Aspergillus airway colonization and invasive disease after lung transplantation. Chest 1997; 112(5): 1160–4.
- Phoompoung P, Villalobos APC, Jain S, Foroutan F, Orchanian-Cheff A, Husain S. Risk factors of invasive fungal infections in lung transplant recipients: A systematic review and meta-analysis. J Heart Lung Transplant 2022; 41(2): 255–62.
- Aguilar CA, Hamandi B, Fegbeutel C, et al. Clinical risk factors for invasive aspergillosis in lung transplant recipients: Results of an international cohort study. J Heart Lung Transplant 2018; 37(10): 1226–34.
- Sole A, Morant P, Salavert M, Peman J, Morales P, Valencia Lung Transplant G. Aspergillus infections in lung transplant recipients: risk factors and outcome. Clin Microbiol Infect 2005; 11(5): 359–65.
- Weigt SS, Elashoff RM, Huang C, et al. Aspergillus colonization of the lung allograft is a risk factor for bronchiolitis obliterans syndrome. Am J Transplant 2009; 9(8): 1903–11.
- Le Pavec J, Pradere P, Gigandon A, et al. Risk of Lung Allograft Dysfunction Associated With Aspergillus Infection. Transplant Direct 2021; 7(3): e675.
- Pennington KM, Yost KJ, Escalante P, Razonable RR, Kennedy CC. Antifungal prophylaxis in lung transplant: A survey of United States' transplant centers. Clin Transplant 2019; 33(7): e13630.
- Husain S, Sole A, Alexander BD, et al. The 2015 International Society for Heart and Lung Transplantation Guidelines for the management of fungal infections in mechanical circulatory support and cardiothoracic organ transplant recipients: Executive summary. J Heart Lung Transplant 2016; 35(3): 261–82.
- Pennington KM, Baqir M, Erwin PJ, Razonable RR, Murad MH, Kennedy CC. Antifungal prophylaxis in lung transplant recipients: A systematic review and meta-analysis. Transpl Infect Dis 2020; 22(4): e13333.
- Patterson TF, Thompson GR, 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis 2016; 63(4): e1–e60.
- Tofte N, Jensen C, Tvede M, Andersen CB, Carlsen J, Iversen M. Use of prophylactic voriconazole for three months after lung transplantation does not reduce infection with Aspergillus: a retrospective study of 147 patients. Scand J Infect Dis 2012; 44(11): 835–41.
- Minari A, Husni R, Avery RK, et al. The incidence of invasive aspergillosis among solid organ transplant recipients and implications for prophylaxis in lung transplants. Transpl Infect Dis 2002; 4(4): 195–200.
- Monforte V, Roman A, Gavalda J, et al. Nebulized amphotericin B prophylaxis for Aspergillus infection in lung transplantation: study of risk factors. J Heart Lung Transplant 2001; 20(12): 1274–81.
- Gemert JPV, Fleurke GJ, Akkerman OW, et al. Aspergillus After Lung Transplantation: Prophylaxis, Risk Factors, and the Impact on Chronic Lung Allograft Dysfunction. Transpl Infect Dis 2025; 27(4): e70020.
- De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 2008; 46(12): 1813–21.
- Husain S, Mooney ML, Danziger-Isakov L, et al. A 2010 working formulation for the standardization of definitions of infections in cardiothoracic transplant recipients. J Heart Lung Transplant 2011; 30(4): 361–74.
- Pinney MF, Rosenberg AF, Hampp C, Schain D, Akindipe O, Baz M. Invasive fungal infections in lung transplant recipients not receiving routine systemic antifungal prophylaxis: 12-year experience at a university lung transplant center. Pharmacotherapy 2011; 31(6): 537–45.
- Husain S, Bhaskaran A, Rotstein C, et al. A strategy for prevention of fungal infections in lung transplantation: Role of bronchoalveolar lavage fluid galactomannan and fungal culture. J Heart Lung Transplant 2018; 37(7): 886–94.
- Gemert JPV, Fleurke GJ, Akkerman OW, et al. Aspergillus After Lung Transplantation: Prophylaxis, Risk Factors, and the Impact on Chronic Lung Allograft Dysfunction. Transpl Infect Dis 2025: e70020.
- Luong ML, Chaparro C, Stephenson A, et al. Pretransplant Aspergillus colonization of cystic fibrosis patients and the incidence of post-lung transplant invasive aspergillosis. Transplantation 2014; 97(3): 351–7.
- Linder KA, Kauffman CA, Patel TS, Fitzgerald LJ, Richards BJ, Miceli MH. Evaluation of targeted versus universal prophylaxis for the prevention of invasive fungal infections following lung transplantation. Transplant Infectious Disease 2021; 23(1).
- Husain S, Kwak EJ, Obman A, et al. Prospective assessment of Platelia Aspergillus galactomannan antigen for the diagnosis of invasive aspergillosis in lung transplant recipients. Am J Transplant 2004; 4(5): 796–802.
- Morgan J, Wannemuehler KA, Marr KA, et al. Incidence of invasive aspergillosis following hematopoietic stem cell and solid organ transplantation: interim results of a prospective multicenter surveillance program. Med Mycol 2005; 43 Suppl 1: S49–58.
- Husain S, Paterson DL, Studer S, et al. Voriconazole prophylaxis in lung transplant recipients. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons 2006; 6(12): 3008–16.
- Iversen M, Burton CM, Vand S, et al. Aspergillus infection in lung transplant patients: incidence and prognosis. Eur J Clin Microbiol Infect Dis 2007; 26(12): 879–86.
- Arthurs SK, Eid AJ, Deziel PJ, et al. The impact of invasive fungal diseases on survival after lung transplantation. Clin Transplant 2010; 24(3): 341–8.
- Eriksson M, Lemström K, Suojaranta-Ylinen R, et al. Control of early Aspergillus mortality after lung transplantation: outcome and risk factors. Transplant Proc 2010; 42(10): 4459–64.
- Koo S, Kubiak DW, Issa NC, et al. A targeted peritransplant antifungal strategy for the prevention of invasive fungal disease after lung transplantation: a sequential cohort analysis. Transplantation 2012; 94(3): 281–6.
- Neoh CF, Snell GI, Levvey B, et al. Preemptive treatment with voriconazole in lung transplant recipients. Transpl Infect Dis 2013; 15(4): 344–53.
- He X, Dai HP, Chen QR, et al. Pneumonia relevant to lung transplantation and pathogen distribution. Chin Med J (Engl) 2013; 126(17): 3209–14.
- Neofytos D, Treadway S, Ostrander D, et al. Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: a 10-year, single-center experience. Transpl Infect Dis 2013; 15(3): 233–42.
- Doligalski CT, Benedict K, Cleveland AA, et al. Epidemiology of invasive mold infections in lung transplant recipients. Am J Transplant 2014; 14(6): 1328–33.
- Vazquez R, Vazquez-Guillamet MC, Suarez J, Mooney J, Montoya JG, Dhillon GS. Invasive mold infections in lung and heart-lung transplant recipients: Stanford University experience. Transpl Infect Dis 2015; 17(2): 259–66.
- Jeong W, Snell GI, Levvey BJ, et al. Clinical effectiveness of early posaconazole suspension pre-emptive therapy in lung transplant recipients: The Alfred's experience. J Antimicrob Chemother 2017; 72(7): 2089–92.
- Herrera S, Davoudi S, Farooq A, et al. Late Onset Invasive Pulmonary Aspergillosis in Lung Transplant Recipients in the Setting of a Targeted Prophylaxis/Preemptive Antifungal Therapy Strategy. Transplantation 2020; 104(12): 2575–81.
- Cadena J, Levine DJ, Angel LF, et al. Antifungal prophylaxis with voriconazole or itraconazole in lung transplant recipients: hepatotoxicity and effectiveness. Am J Transplant 2009; 9(9): 2085–91.
- Pasqualotto AC, Xavier MO, Sánchez LB, et al. Diagnosis of invasive aspergillosis in lung transplant recipients by detection of galactomannan in the bronchoalveolar lavage fluid. Transplantation 2010; 90(3): 306–11.
- Hosseini-Moghaddam SM, Chaparro C, Luong M-L, et al. The Effectiveness of Culture-Directed Preemptive Anti-Aspergillus Treatment in Lung Transplant Recipients at One Year After Transplant. Transplantation 2015; 99(11): 2387–93.
- Alissa D, AlMaghrabi R, Nizami I, et al. Nebulized Amphotericin B Dosing Regimen for Aspergillus Prevention After Lung Transplant. Exp Clin Transplant 2021; 19(1): 58–63.
- Le Pavec J, Pradère P, Gigandon A, et al. Risk of Lung Allograft Dysfunction Associated With Aspergillus Infection. Transplant Direct 2021; 7(3): e675.
- Villalobos AP, Foroutan F, Davoudi S, et al. Statin Use May Be Associated With a Lower Risk of Invasive Aspergillosis in Lung Transplant Recipients. Clin Infect Dis 2023; 76(3): e1379–e84.
- Crone CG, Wulff SM, Ledergerber B, et al. Invasive Aspergillosis among Lung Transplant Recipients during Time Periods with Universal and Targeted Antifungal Prophylaxis-A Nationwide Cohort Study. J Fungi (Basel) 2023; 9(11).
- Crone CG, Wulff SM, Helweg-Larsen J, et al. Adverse Events Associated with Universal versus Targeted Antifungal Prophylaxis among Lung Transplant Recipients-A Nationwide Cohort Study 2010-2019. Microorganisms 2022; 10(12).
- Ascioglu S, Rex JH, de Pauw B, et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis 2002; 34(1): 7–14.
- Baker AW, Maziarz EK, Arnold CJ, et al. Invasive Fungal Infection After Lung Transplantation: Epidemiology in the Setting of Antifungal Prophylaxis. Clin Infect Dis 2020; 70(1): 30–9.
- Huggins JP, Arthur D, Chow SC, et al. Risk Factors for Invasive Fungal Infection in Lung Transplant Recipients on Universal Antifungal Prophylaxis. Open Forum Infect Dis 2024; 11(2): ofad640.
- Umemura K, Katada Y, Nakagawa S, et al. Comparison of the safety and cost-effectiveness of nebulized liposomal amphotericin B and amphotericin B deoxycholate for antifungal prophylaxis after lung transplantation. JOURNAL OF INFECTION AND CHEMOTHERAPY 2024; 30(8): 741–5.
- Monforte V, Ussetti P, Gavaldà J, et al. Feasibility, tolerability, and outcomes of nebulized liposomal amphotericin B for Aspergillus infection prevention in lung transplantation. The Journal of Heart and Lung Transplantation 2010; 29(5): 523–30.
- Drew RH, Dodds Ashley E, Benjamin DK, Jr., Duane Davis R, Palmer SM, Perfect JR. Comparative safety of amphotericin B lipid complex and amphotericin B deoxycholate as aerosolized antifungal prophylaxis in lung-transplant recipients. Transplantation 2004; 77(2): 232–7.
- Lowry CM, Marty FM, Vargas SO, et al. Safety of aerosolized liposomal versus deoxycholate amphotericin B formulations for prevention of invasive fungal infections following lung transplantation: a retrospective study. Transpl Infect Dis 2007; 9(2): 121–5.
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 2020; 71(6): 1367–76.
- Ju C, Lian Q, Chen A, et al. Antifungal prophylactic effectiveness and intrapulmonary concentrations of voriconazole versus posaconazole in lung transplant recipients. Med Mycol 2022; 60(9).
- Pennington KM, Razonable RR, Peters S, et al. Why do lung transplant patients discontinue triazole prophylaxis? Transpl Infect Dis 2019; 21(3): e13067.
- Hamandi B, Fegbeutel C, Silveira FP, et al. Voriconazole and squamous cell carcinoma after lung transplantation: A multicenter study. Am J Transplant 2018; 18(1): 113–24.
- D'Arcy ME, Pfeiffer RM, Rivera DR, et al. Voriconazole and the Risk of Keratinocyte Carcinomas Among Lung Transplant Recipients in the United States. JAMA Dermatol 2020; 156(7): 772–9.
- Vadnerkar A, Nguyen MH, Mitsani D, et al. Voriconazole exposure and geographic location are independent risk factors for squamous cell carcinoma of the skin among lung transplant recipients. J Heart Lung Transplant 2010; 29(11): 1240–4.
- Feist A, Lee R, Osborne S, Lane J, Yung G. Increased incidence of cutaneous squamous cell carcinoma in lung transplant recipients taking long-term voriconazole. J Heart Lung Transplant 2012; 31(11): 1177–81.
- Mansh M, Binstock M, Williams K, et al. Voriconazole Exposure and Risk of Cutaneous Squamous Cell Carcinoma, Aspergillus Colonization, Invasive Aspergillosis and Death in Lung Transplant Recipients. Am J Transplant 2016; 16(1): 262–70.
- Singer JP, Boker A, Metchnikoff C, et al. High cumulative dose exposure to voriconazole is associated with cutaneous squamous cell carcinoma in lung transplant recipients. J Heart Lung Transplant 2012; 31(7): 694–9.
- Thakuria L, Packwood K, Firouzi A, et al. A pharmacokinetic analysis of posaconazole oral suspension in the serum and alveolar compartment of lung transplant recipients. Int J Antimicrob Agents 2016; 47(1): 69–76.
- Zhang H, Nguyen MH, Clancy CJ, et al. Pharmacokinetics of Posaconazole Suspension in Lung Transplant Patients with and without Cystic Fibrosis. Antimicrob Agents Chemother 2016; 60(6): 3558–62.
- Launay M, Roux A, Beaumont L, et al. Posaconazole Tablets in Real-Life Lung Transplantation: Impact on Exposure, Drug-Drug Interactions, and Drug Management in Lung Transplant Patients, Including Those with Cystic Fibrosis. Antimicrob Agents Chemother 2018; 62(3).
- Hurtik R, Bag R, Neujahr DC. Acheiving Therapeutic Posaconazole Levels for Fungal Prophylaxis After Lung Transplantation; Oral Suspension Versus Delayed-Release Tablets. The Journal of Heart and Lung Transplantation 2015; 34(4): S55.
- Nguyen MH, Davis MR, Wittenberg R, et al. Posaconazole Serum Drug Levels Associated With Pseudohyperaldosteronism. Clin Infect Dis 2020; 70(12): 2593–8.
- Chen B, Trang V, Lee A, et al. Posaconazole, a Second-Generation Triazole Antifungal Drug, Inhibits the Hedgehog Signaling Pathway and Progression of Basal Cell Carcinoma. Mol Cancer Ther 2016; 15(5): 866–76.
- Whitmore TJ, Yaw M, Lavender M, Musk M, Boan P, Wrobel J. A novel highly bio-available itraconazole formulation (SUBA(R)-Itraconazole) for anti-fungal prophylaxis in lung transplant recipients. Transpl Infect Dis 2021; 23(4): e13587.
- Kallee S, Scharf C, Schroeder I, et al. Comparing posaconazole and itraconazole for antifungal prophylaxis in critically ill lung transplant recipients: Efficacy and plasma concentrations. Transpl Infect Dis 2021; 23(4): e13675.
- Kennedy CC, Razonable RR. Fungal Infections After Lung Transplantation. Clin Chest Med 2017; 38(3): 511–20.
- Al Jishi Y, Rotstein C, Kumar D, et al. Echinocandin use in lung transplant recipients. Clin Transplant 2018; 32(12): e13437.
- Sartain E, Schoeppler K, Crowther B, et al. Perioperative anidulafungin combined with triazole prophylaxis for the prevention of early invasive candidiasis in lung transplant recipients. Transpl Infect Dis 2021; 23(4): e13692.
- Pasley T, Baladad C, DeSear K, et al. Bridging Echinocandin With Azole Antifungal Therapy on Prevention of Invasive Candidiasis Post-Lung Transplantation. Open Forum Infect Dis 2024; 11(9): ofae525.
- Boscolo A, Cattelan A, Marinello S, et al. Fungal Infections and Colonization after Bilateral Lung Transplant: A Six-Year Single-Center Experience. J Fungi (Basel) 2024; 10(1).
- Ju C, Lian Q, Wang X, et al. Efficacy of different durations of antifungal prophylaxis with nebulized amphotericin B after lung transplantation: a retrospective cohort study. J Thorac Dis 2023; 15(10): 5396–404.
- Young JH, Andes DR, Ardura MI, et al. Modeling Invasive Aspergillosis Risk for the Application of Prophylaxis Strategies. Open Forum Infect Dis 2024; 11(3): ofae082.
- Shields RK, Nguyen MH, Shullo MA, et al. Invasive aspergillosis among heart transplant recipients is rare but causes rapid death due to septic shock and multiple organ dysfunction syndrome. Scand J Infect Dis 2012; 44(12): 982–6.
- Tissot F, Pascual M, Hullin R, et al. Impact of targeted antifungal prophylaxis in heart transplant recipients at high risk for early invasive fungal infection. Transplantation 2014; 97(11): 1192–7.
- Rabin AS, Givertz MM, Couper GS, et al. Risk factors for invasive fungal disease in heart transplant recipients. J Heart Lung Transplant 2015; 34(2): 227–32.
- Echenique IA, Angarone MP, Gordon RA, et al. Invasive fungal infection after heart transplantation: A 7-year, single-center experience. Transpl Infect Dis 2017; 19(1).
- Cook JC, Cook A, Tran RH, Chang PP, Rodgers JE. A case-control study of the risk factors for developing aspergillosis following cardiac transplant. Clin Transplant 2018; 32(9): e13367.
- Chheda JJ, Tarleton A, Eidem JH. Targeted Aspergillus Prophylaxis With Voriconazole in Heart Transplant Patients: A Focus on the Interaction With Tacrolimus. J Pharm Technol 2019; 35(4): 164–71.
- Perry WA, Chow JK, Nelson J, Kent DM, Snydman DR. A Clinical Model to Predict the Occurrence of Select High-risk Infections in the First Year Following Heart Transplantation. Transplant Direct 2023; 9(12): e1542.
- Küpeli E, Ulubay G, Bayram Akkurt S, Öner Eyüboğlu F, Sezgin A. Invasive pulmonary aspergillosis in heart transplant recipients. Exp Clin Transplant 2015; 13 Suppl 1: 352–5.
- Paniagua Martin MJ, Marzoa Rivas R, Barge Caballero E, et al. Efficacy and tolerance of different types of prophylaxis for prevention of early aspergillosis after heart transplantation. Transplant Proc 2010; 42(8): 3014–6.
- Montoya JG, Chaparro SV, Celis D, et al. Invasive aspergillosis in the setting of cardiac transplantation. Clin Infect Dis 2003; 37 Suppl 3: S281–92.
- Muñoz P, Rodríguez C, Bouza E, et al. Risk factors of invasive aspergillosis after heart transplantation: protective role of oral itraconazole prophylaxis. Am J Transplant 2004; 4(4): 636–43.
- Utili R, Zampino R, De Vivo F, et al. Improved outcome of pulmonary aspergillosis in heart transplant recipients with early diagnosis and itraconazole treatment. Clin Transplant 2000; 14(4 Pt 1): 282–6.
- van Delden C, Stampf S, Hirsch HH, et al. Burden and Timeline of Infectious Diseases in the First Year After Solid Organ Transplantation in the Swiss Transplant Cohort Study. Clin Infect Dis 2020; 71(7): e159–e69.
- Yetmar ZA, Lahr B, Brumble L, et al. Epidemiology, risk factors, and association of antifungal prophylaxis on early invasive fungal infection in heart transplant recipients. Transpl Infect Dis 2021; 23(5): e13714.
- Gavalda J, Len O, San Juan R, et al. Risk factors for invasive aspergillosis in solid-organ transplantrecipients: a case-control study. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 2005; 41(1): 52–9.
- Segal BH, Herbrecht R, Stevens DA, et al. Defining responses to therapy and study outcomes in clinical trials of invasive fungal diseases: Mycoses Study Group and European Organization for Research and Treatment of Cancer consensus criteria. Clin Infect Dis 2008; 47(5): 674–83.
List of Abbreviations
AEs: Adverse events
AAP: The American Academy of Pediatrics
ABLC: Amphotericin B lipid complex
AC: Acquisition cost
AFT: Antifungal therapy
AmB: Amphotericin B
aOR: Adjusted odds ratio
aRR: Adjusted risk ratio
ASCO: The American Society of Clinical Oncology
AST: The American Society of Transplantation
AWP: Average wholesale prices
BD: Twice a day
CAR: Chimeric antigen receptor
CI: Confidence interval
CMV: Cytomegalovirus
CNI: Calcineurin inhibitor
COE: Certainty of evidence
COI: Conflict of interest
CRRT: Continuous renal replacement therapy
d-AmB: Amphotericin B deoxycholate
EORTC/MSG: The European Organization for Research and Treatment of Cancer/Mycoses Study Group
GGT: Gamma-glutamyl transpeptidase enzyme
GI: Gastrointestinal system
GLMM: Generalized linear mixed-effects model
GRADE: Grading of Recommendations Assessment, Development and Evaluation
HCT: Hematopoietic cell transplant
HM: Hematologic malignancy
IA: Invasive aspergillosis
IC: Invasive candidiasis
ICD-9: The International Classification of Diseases, Ninth Revision
ICU: Intensive care unit
IDSA: The Infectious Disease Society of America
IFIs: Invasive fungal infections
IMIs: Invasive mold infections
IPA: Invasive pulmonary aspergillosis
IQR: Interquartile range
ISHLT: The International Society for Heart and Lung Transplantation
IV: Intravenous route
KP: Kidney pancreas transplant
L-AmB: Liposomal amphotericin B
MID: Minimal important difference
mITT: Modified intent-to-treat
NR: Not reported
OLT: orthotopic liver transplant
OR: Odds ratio
PAK: Pancreas after kidney transplant
PCR: Polymerase chain reaction
PICO: Patient/Population; Intervention/Indicator; Comparator/Control; Outcome
PO: Oral route
PP: Per protocol
PRISMA: Preferred reporting items for systematic reviews and meta-analyses
PSID: The Pediatric Infectious Disease Society
PTA: Pancreas transplant alone
RCT: Randomized clinical trials or randomized controlled trials
RD: Risk difference
RF: Risk factor
RR: Relative risk
RRT: Renal replacement therapy
QTc: QT interval corrected
SEA: Serious adverse events
SARS-CoV2: severe acute respiratory syndrome coronavirus 2
SOT: Solid organ transplant
SPGS: The Standards and Practice Guideline Subcommittee
SPK: Simultaneous pancreas kidney transplant
TDA: Three times a day
TDM: Therapeutic drug monitoring
Acknowledgments
First, the panel would like to acknowledge the previous panel for their work on the previous iteration of this larger guideline. The panel would like to acknowledge the important contributions of Mary Beth McAteer (librarian supporting systematic and mapping reviews), Loretta Dzanya (IDSA staff assisting with logistics and editorial coordination) and Malavika Tampi (previous IDSA methodologist helping with the development of clinical questions). The panel would also like to acknowledge the following organizations and selected primary (SPGS) and external reviewers for their review of the draft manuscripts: The American Academy of Pediatrics (AAP), The American Society of Clinical Oncology (ASCO), The American Society of Transplantation (AST), The Pediatrics Infectious Diseases Society (PIDS), Drs. Emily Blumberg, Jennifer Saullo, Lianne Singer, Peter Pappas, Shmuel Shoham, and Surabhi (Sara) Vora.
Dr. Mindy G. Schuster is the Chair of the Aspergillosis Guideline Panel, and Dr. C. Orla Morrissey is the Vice Chair of the panel. Drs. Jo-Anne H, M. Hong Nguyen, Nitipong Permpalung, and Shahid M. Husain for their leading role in the development of Adult Solid Organ Transplant Recipients section of the Clinical Practice Guidelines on Prevention of Invasive Aspergillosis. The remaining panelists contributed to the conception and design of the analysis, interpretation of the data, drafting and revision of the recommendations and manuscript, and final approval of the published recommendations and manuscript. Dr. Valéry Lavergne, IDSA clinical practice guidelines senior methodologist, was responsible for overall project management, designing and conducting the systematic review, and leading the panel in accordance with the GRADE process, developing the manuscript and curating the supplementary material.
Conflicts of Disclosure
Possible conflicts of interest. Evaluation of relationships as potential conflicts of interest is determined by a review process. The assessment of disclosed relationships for possible COIs is based on the relative weight of the financial relationship (i.e., monetary amount) and the relevance of the relationship (i.e., the degree to which an association might reasonably be interpreted by an independent observer as related to the topic or recommendation of consideration).
The following panelists have reported relationships unrelated to the topic of fungal infections/antifungal therapies since 2021–2025, when the guideline work began, with the indicated companies. S.H. received educational grants and served in advisory roles with Takeda, Xedition, Kamada, Knight Therapeutic, Sanofi, and GSK for unrelated topics; served in editorial roles with the Journal of Heart and Lung Transplantation and Transplant Infectious Diseases. N.P. served in past advisory/consulting roles with ClearView and Alcimed (unrelated); held editorial roles with Medical Mycology and the Journal of Heart and Lung Transplantation Open. M.H.N. received research grants from bioMérieux (target NGS for fungal diagnosis direct from samples) and Melinta (Rezafungin clinical trial). J.H.Y. received research funding for subject enrollment on clinical trials from AlloVir (adoptive T cells) and Ansun (DAS-181 for viral infections); served as Editor-in-Chief for Clinical Microbiology Reviews; serves as an Associate Editor for Transplantation and Cellular Therapy; receives research funding for subject enrollment on clinical trials from AiCuris (HSV infection), GSK (RSV vaccination), Lumen (C diff infection), Pulmotect (respiratory viral infections), SNIPR (phage therapy), Shire/Takeda (CMV infection), and Vedanta (C diff infection). M.S. received funding from the Public Health Agency of Canada for initiatives related to antimicrobial stewardship. D.R.A. served in advisory roles for Roche, Basilea, Cidara, Astellas, Mundipharma, F2G, Amplyx, and Elion; owned stock in Symbiotica; served on the editorial board for Clinical Infectious Diseases/Journal of Infectious Diseases (CID/JID) as editor for Antimicrobial Agents and Chemotherapy (AAC), Journal of Infectious Diseases, mBio, and PLoS Pathogens; served as a member for the Clinical and Laboratory Standards Institute (CLSI). M.I.A. served as a consultant for Karius (application of Karius for fungal diagnostics in immunocompromised children); Miravista (evaluating fungal diagnostics in children with research support paid to institution); received travel reimbursement from St. Jude Children’s Research Hospital (participation in infectious disease research conferences); serves as an editorial board member for Transplant Infectious Disease and the Journal of the Pediatric Infectious Diseases Society; serves on the American Academy of Pediatrics (AAP) Committee on Infectious Diseases). E.J.B. served in advisory roles for Avir Pharma and GSK; participates as a guidelines panel member for the American Society of Clinical Oncology and Infectious Diseases Society of America (neutropenic fevers); received honoraria as Section Editor, Up-to-Date. P.H.C. participated in a speakers bureau for Astellas (isavuconazole); received research funding from Aicuris (recruited patients for HSV Pritelevir study); received other remuneration from Pfizer (data review on Aztreonam-Avibactam study); served as president at Michigan State Infectious Diseases Society; serves as editor at the British Journal of Antimicrobial Agents and Chemotherapy. S.C-A.C. received organizational benefits from MSD Australia (untied educational grants); served as Pathology editor for the Journal of Clinical Microbiology, editor for Microbiology, editor-in-chief for Medical Mycology, and as a board member for the Mycoses Study Group Education and Research Consortium (MSGERC). S.P.H. served in past advisory and consulting roles with Pfizer (advisory roles regarding infections associated with BCMA bispecific antibodies and myeloma therapies), Roche (advisory board regarding infectious complications of therapies for multiple myeloma), Treeline Biosciences (consulting regarding infectious complications of novel targets therapies for lymphoma) and Seres Therapeutics (consulting regarding infectious complications of leukemia therapy and use of live spore products in hematologic malignancy patients) ; received research funding from GlaxoSmithKline (GSK) for a study of sotrovimab prophylaxis against COVID-19 infection in immunocompromised individuals; serves in an advisory role (scientific) with Takeda (infection adjudication committee for a clinical trial). S.A.K. reported family relationships (spouse consulting roles or employment) with Boston Scientific, Janssen, Novartis, Myovant, Blue Earth Diagnostics, MDx Health, AIQ, Reversal Therapeutics, Stratagen Bio, and Nanocan; received research funding from GlaxoSmithKline (GSK); serves in an advisory role with Vertex Pharmaceuticals (member of a safety adjudication committee for a clinical trial; unrelated). G.R.T. served in advisory as a consultant for Cidara (clinical trial design). M.G.S. served as associate editor for Annals of Internal Medicine (American College of Physicians). V.L. received funding from Centre de Recherche du Centre Intégré Universitaire de Santé et de Services Sociaux du Nord-de-l’île-de-Montréal (CIUSSS_NIM).
The following panelists have reported relationships related to the topic of fungal infections/antifungal therapies since 2021–2025, when the guideline work began, with the indicated companies. S.H. received educational grants from Merck (posaconazole), Astellas , Avir Pharma, Sanofi, and GlaxoSmithKline (GSK); served in advisory roles with TFF Pharmaceuticals (inhaled voriconazole), Takeda (Maribavir), ITB Med (siplizumab), and TFF Pharmaceuticals; received research funding from the National Institutes of Health, University Health Network, Princess Margaret Hospital Foundation, PSI Foundation (PC945 studies), Scynexis (Ibrexafungerp studies), Pulmocide (opelconazole studies), F2G (olorofim studies), Baselia (Fosmanogepix) and Gilead (immunomodulatory effects of antifungals) (all paid to institution); served in an editorial role as section editor for the Journal of Heart and Lung Transplantation and Transplant Infectious Diseases. N.P. served in advisory roles for Pulmocide (opelconazole) and Basilea (Fosmanogepix); received research funding from Scynexis (candidemia/invasive candidiasis studies), Merck (long-term outcomes of SARS-CoV-2 infections and COVID-19 vaccine breakthrough risk in kidney transplant recipients – clinical burden of RSV and other respiratory viral infections in immunocompromised hosts), CareDx, Inc. (kidney allograft outcomes, Allosure registry), Pulmocide Ltd (opelconazole clinical trials), IMMY Diagnostics (Aspergillus galactomannan assay evaluation), Pearl Diagnostics (urine MycoMEIA), Applied BioCode (ABC assay), Fujifilm (Beta-d-glucan), Zepto Life Technology (cfDNA) and the Cystic Fibrosis Foundation, National Institutes of Health, Health Systems Research Institute, and Chulalongkorn University (various studies on fungal infections, transplant outcomes, and infectious disease diagnostics). M.H.N. received research funding from NIH/NIAID and CDC/Mycoses Study Group, investigator-initiated research grants from bioMérieux (target NGS for fungal diagnosis direct from samples) and Melinta (Rezafungin clinical trial), clinical trial funding from F2G Ltd UK (olorofim) and Pulmocide (opelconazole); all funds were paid directly to the University of Pittsburgh; serves on the advisory board for Basilea Pharmaceutica International Ltd (Fosmanogepix) and Pulmocide (opelconazole). J.H.Y. received research funding for subject enrollment on clinical trials from Basilea (Fosmanogepix), Cidara/Mundipharma (Rezafungin), F2G (olorofim), and Scynexis (Ibrexafungerp); received industry support from the NIH for studies related to antifungal and infectious disease therapeutics; receives research funding for subject enrollment on clinical trials from Pulmocide (opelconazole) and Zepto (fungal diagnostics); serves on the Aspergillus Guidelines panel with the European Confederation of Medical Mycology. M.I.A. received research funding and remuneration related to antifungal/viral therapeutics from Merck (letermovir), Shire (maribavir), and Miravista (Histoplasma diagnostics); received research funding from NIH (comparison of high dose vs standard dose influenza vaccine in HCT recipients – multicenter prospective study of human adenovirus infection and disease in pediatric HCT recipients and non-invasive diagnosis of pediatric pulmonary invasive mold infection); served as a consultant for Karius (diagnostics). A.C.A. received research funding from Merck, Astellas, Nabriva, Paratek, and Summit Therapeutics for clinical trials involving antifungal and antibacterial agents. A past speaking engagement with Astellas (Sept 2025–Feb 2026), related to a product in scope, was also reported. However, A.C.A.’s role in the guideline development was limited; he was not part of the core subgroup, did not advocate for specific therapies, and contributed only minor technical input. S.C-A.C. received research funding from F2G, Pfizer Australia for studies involving fungal infections, and prior funding from PRSP for infectious disease surveillance including mycology. S.P.H. served in advisory roles for F2G (olorofim) and Melinta (Rezafungin); received research funding from F2G, Scynexis, Mundipharma, Cidara, and Elion related to antifungal therapeutics (all paid to institution). S.A.K. received research funding from Scynexis and GSK related to antifungal and infectious disease therapeutics; received research funding from the NIH for work related to pneumonia diagnostics. T.F.P. served in advisory and consulting roles for F2G (olorofim and other investigational antifungals), Basilea (isavuconazole and Fosmanogepix), Gilead (amBisome), Pfizer (voriconazole), Scynexis (Ibrexafungerp), and Sfunga (investigational antifungals); received research funding from the National Institutes of Health (including RECOVER, ACTT/ACTIV, U19 Coccidioidomycosis Research Center, STOMP, and preclinical infectious disease studies); received industry sponsorship from F2G (olorofim for resistant molds) and Cidara (Rezafungin). G.R.T. served in advisory roles for Astellas, Basilea, Elion, F2G, GSK, and Cidara related to antifungal agents (e.g., isavuconazole, olorofim, Fosmanogepix, Turletricin, Rezafungin, Ibrexafungerp); receives research funding from F2G (OASIS) and Astellas (Mycoses Study Group; Radiology Study). C.O.M. served in advisory roles for Gilead Sciences (liposomal amphotericin B), Merck Sharp & Dohme, Australia (caspofungin and posaconazole), Pfizer, Australia (voriconazole and anidulafungin) and Elio Therapeutics (SF001); received honoraria from Gilead Sciences (webinar chair, liposomal amphotericin B), Merck Sharp & Dohme, Australia (fungal diagnostics), and Pfizer, Australia (diagnostic stewardship); received research funding from F2G Ltd UK (F901318), Cidara Therapeutics Inc. (Rezafungin), Gilead Sciences (azole resistance studies), and Merck Sharp & Dohme, Australia (UPPRITE trial and posaconazole use in cystic fibrosis), all funding paid directly to institution. All other authors reported no conflicts of interest during the specified period.
Publication Disclaimer
©IDSA<2026>. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, transmitted, used for text and data mining, or used for training artificial intelligence, in any form or by any means, without the prior permission in writing, or as expressly permitted by law, by license or under terms agreed with the appropriate reprographics rights organization. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through the Oxford University Press RightsLink service via the Permissions link for this paper in Clinical Infectious Diseases. For further information please contact journals.permissions@oup.com.
Update History
As of June 26, 2026, the Infectious Diseases Society of America (IDSA) has released updated recommendations for the diagnosis and management of aspergillosis, replacing the previous guidelines last updated in 2016. The current guidelines are available on the IDSA website and will be published in Clinical Infectious Diseases (CID) at a later date.