July 30, 2026
The Infectious Diseases Society of America (IDSA) is committed to delivering timely, evidence-informed guidance on the management of antimicrobial-resistant (AMR) infections. This updated IDSA AMR Guidance document provides treatment suggestions for infections caused by extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E), AmpC β-lactamase–producing Enterobacterales (AmpC-E), carbapenem-resistant Enterobacterales (CRE), Pseudomonas aeruginosa with difficult-to-treat resistance (DTR P. aeruginosa), carbapenem-resistant Acinetobacter baumannii (CRAB), and Stenotrophomonas maltophilia. This update replaces earlier versions of the IDSA AMR Treatment Guidance.
Please submit your feedback and comments on the AMR Guidance by emailing us at PracticeGuidelines@idsociety.org.
Pranita D. Tamma*, Robert A. Bonomo, Emily L. Heil, Julie Ann Justo, Michael J. Satlin, & Amy J. Mathers
*Corresponding Author: Pranita D. Tamma, MD, MHS, University of Pennsylvania School of Medicine, Department of Pediatrics, Philadelphia, Pennsylvania, USA; Pranita.Tamma@PennMedicine.upenn.edu
Keywords: ESBL; AmpC; carbapenem-resistant Enterobacterales; Pseudomonas aeruginosa; CRAB; Stenotrophomonas maltophilia
Update History
August 7, 2024
Version 4.0 of the guidance has been released.
Notable Updates from the 2024 IDSA AMR Guidance Document
The reader is encouraged to review the entire AMR Guidance document as edits and updated pre-clinical and clinical data have been made to most questions.
Introduction
- Updated projections describing the burden of morbidity and mortality attributable to antimicrobial resistance (AMR).
- Harmonized definitions of uncomplicated and complicated urinary tract infections with the 2025 IDSA Guidelines on the Management and Treatment of Complicated Urinary Tract Infections.
- Added a reference outlining dosing recommendations for newer β-lactam agents based on a consensus statement from United States pediatric infectious diseases pharmacists to provide suggested dosing of antibiotics for AMR infections in children.
- Added clarifying language indicating that preferred and alternative antibiotic options are presented in alphabetical order within the “Suggested Approach” sections; additional nuance regarding prioritization among agents is provided in the corresponding “Rationale” sections.
- Updated Table 1 (antibiotic dosing suggestions) to reflect the most current available evidence.
- Updated Table 2 with 2026 CLSI antibiotic susceptibility breakpoint data.
- Updated the Supplemental Material to align with the updated Table 1.
Extended-spectrum β-lactamase-producing Enterobacterales (ESBL-E)
- Revised the criteria for presumed ESBL production in E. coli, K. pneumoniae, and K. oxytoca to ceftriaxone MIC ≥4 µg/mL, reflecting updated evidence.
- Updated estimates of the prevalence of ESBL production among E. coli isolates in the United States.
- Added references describing the molecular epidemiology and species-specific prevalence of non-CTX-M ESBL enzymes.
- Added information regarding the FDA-approved agent gepotidacin for the treatment of ESBL-E infections.
- Added information regarding the FDA-approved agent pivmecillinam for the treatment of ESBL-E infections.
- Added information regarding the FDA-approved agent oral sulopenem for the treatment of ESBL-E infections.
- Added information on the suggested role of cefepime-enmetazobactam for the treatment of ESBL-E infections.
- Added information regarding the FDA-approved agent intravenous fosfomycin for the treatment of ESBL-E infections.
- Expanded discussion of the approximate susceptibility percentages of ESBL-E isolates to non-β-lactam agents used empirically for uncomplicated UTIs.
- Revised suggestions to include piperacillin-tazobactam as an alternative treatment option for complicated UTIs.
- Added references to ongoing clinical trials evaluating piperacillin-tazobactam and cefmetazole (a cephamycin) for the treatment of ESBL-E bloodstream infections.
- Added additional references describing recent comparative effectiveness studies for the treatment of ESBL-E infections.
AmpC-producing Enterobacterales (AmpC-E)
- Updated information regarding the molecular epidemiology of ampC genes in Enterobacterales in the United States.
- Added Hafnia alvei as an organism associated with a moderate risk of clinically significant AmpC production.
- Added language indicating that, in cases of non-severe infection in which ceftriaxone was initiated empirically and the patient demonstrates clinical improvement with adequate source control, continuation of ceftriaxone for completion of therapy may be reasonable.
- Added additional references describing recent comparative effectiveness studies for the treatment of AmpC-E infections.
-
Added additional data supporting the suggestion that piperacillin-tazobactam may be suboptimal for invasive infections caused by Enterobacterales at moderate risk for clinically significant inducible AmpC production.
- Added information regarding the FDA-approved agent gepotidacin for the treatment of AmpC-E infections.
- Added information regarding the FDA-approved agent pivmecillinam for the treatment of AmpC-E infections.
- Added information regarding the FDA-approved agent oral sulopenem for the treatment of AmpC-E infections.
- Added information on the suggested role of cefepime-enmetazobactam for the treatment of AmpC-E infections.
Carbapenem-Resistant Enterobacterales (CRE)
- Updated discussion of the evolving molecular epidemiology of CRE in the United States.
- Added information regarding the FDA-approved agent gepotidacin for the treatment of CRE infections.
- Added information regarding the FDA-approved agent pivmecillinam for the treatment of CRE infections.
- Added information regarding the FDA-approved agent intravenous fosfomycin for the treatment of CRE infections.
- Added information describing susceptibility rates of CRE isolates to non-β-lactam antibiotics that may retain activity against CRE infections.
- Added preclinical and clinical data comparing ceftazidime-avibactam and meropenem-vaborbactam for infections caused by KPC-producing Enterobacterales.
- Added information regarding the FDA-approved agent aztreonam-avibactam for the treatment of NDM-producing infections.
- Added a brief discussion of aztreonam-avibactam and ceftazidime-avibactam plus aztreonam for NDM-producing Enterobacterales, noting either is reasonable for the treatment of NDM-producing Enterobacterales infections, with a slight preference for aztreonam-avibactam.
- Added preclinical and clinical data comparing aztreonam-avibactam and cefiderocol for infections caused by NDM-producing Enterobacterales.
- Updated discussion of known mechanisms of resistance to newer β-lactam agents among CRE isolates.
Pseudomonas aeruginosa with difficult-to-treat resistance (DTR P. aeruginosa)
- Added references describing recent comparative effectiveness studies evaluating ceftazidime-avibactam versus ceftolozane-tazobactam, including data supporting preference for ceftolozane-tazobactam in DTR P. aeruginosa pneumonia.
- Added discussion noting that imipenem-cilastatin-relebactam appears to have a similarly high risk of resistance emergence during therapy as ceftazidime-avibactam and ceftolozane-tazobactam.
- Added data from a clinical trial comparing cefiderocol versus alternative therapy for DTR P. aeruginosa bloodstream infections (i.e., “the Game Changer Trial”).
- Removed the question addressing treatment of uncomplicated UTI caused by DTR P. aeruginosa and added a statement on the suggested approach for this rare scenario at the end of the response to the question regarding treatment of complicated UTI.
- Added a question addressing how identification of carbapenemases in P. aeruginosa should influence treatment selection.
- Updated data describing the emergence of resistance to anti-pseudomonal agents.
-
Updated discussion regarding the role of nebulized antibiotics; while still not routinely preferred, the suggestion against their use was moderated in light of some data suggesting improved clinical cure with their use.
Carbapenem-resistant Acinetobacter baumannii (CRAB) infections
- Added the term “invasive infections” throughout the CRAB section to clarify that suggestions apply to infection rather than colonization.
- Expanded introductory discussion of resistance mechanisms commonly identified in CRAB isolates.
- Removed questions addressing the general treatment approach for CRAB infections and the role of combination therapy.
- Added information regarding the suggested treatment approach for NDM-producing CRAB infections.
- Added language indicating that the priority for invasive CRAB infections is the administration of sulbactam-durlobactam (in combination with a carbapenem) and alternative options should only be administered as bridge therapy until sulbactam-durlobactam is available.
- Added language that if resistance to sulbactam-durlobactam is exhibited, approaches include the use of two non-sulbactam agents or the addition of sulbactam-durlobactam to cefiderocol.
- Added data from a clinical trial comparing cefiderocol versus alternative therapy for CRAB bloodstream infections (i.e., “the Game Changer Trial”).
- Updated data from observational studies evaluating cefiderocol for invasive CRAB infections.
- Removed questions addressing the role of extended-infusion meropenem or imipenem-cilastatin for CRAB infections.
- Removed questions addressing the role of rifamycins for invasive CRAB infections.
-
Updated discussion regarding the role of nebulized antibiotics; while still not routinely preferred, the suggestion against their use was moderated in light of some data suggesting improved clinical cure with their use.
Stenotrophomonas maltophilia Infections
- Removed the question addressing the general treatment approach for infections caused by S. maltophilia.
- Added the term “invasive infections” throughout the section to clarify that suggestions apply to infection rather than colonization.
- Designated cefiderocol monotherapy as the preferred treatment for invasive S. maltophilia infections, with the acknowledgement that this is based on susceptibility data and neutropenic animal studies with very little supportive clinical data.
- Updated data from neutropenic animal studies evaluating the role of cefiderocol in S. maltophilia infections.
-
Changed treatment suggestion to aztreonam-avibactam, preferably in combination with a second agent, is an alternative treatment option for invasive S. maltophilia infections.
- Added data from a clinical trial comparing cefiderocol versus alternative therapy for S. maltophilia bloodstream infections (i.e., “the Game Changer Trial”).
Abstract
Background: The Infectious Diseases Society of America (IDSA) is committed to delivering timely, evidence-informed guidance on the management of antimicrobial-resistant (AMR) infections. This updated IDSA AMR Guidance document provides treatment suggestions for infections caused by extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E), AmpC β-lactamase–producing Enterobacterales (AmpC-E), carbapenem-resistant Enterobacterales (CRE), Pseudomonas aeruginosa with difficult-to-treat resistance (DTR P. aeruginosa), carbapenem-resistant Acinetobacter baumannii (CRAB), and Stenotrophomonas maltophilia. This update replaces earlier versions of the IDSA AMR Treatment Guidance.
Methods: A panel of six infectious diseases specialists with expertise in AMR convened to address important questions regarding the treatment of infections due to ESBL-E, AmpC-E, CRE, DTR P. aeruginosa, CRAB, and S. maltophilia. Given geographic variability in AMR epidemiology and antibiotic availability, the IDSA AMR Guidance focuses on clinical practice in the United States.
Results: Preferred and alternative treatment strategies are outlined with accompanying rationales, based on pathogen identification and in vitro susceptibility data. Suggestions addressing empiric therapy, transition to oral therapy, duration of treatment, and other management considerations are briefly discussed. While applicable to both adult and pediatric populations, specific dosing guidance is only provided for adults.
Conclusions: The field of AMR is highly dynamic. This document is current as of March 1, 2026 and will be updated periodically.
Introduction
Antimicrobial resistance (AMR) represents an escalating global health crisis. In 2019, an estimated 4.95 million deaths were associated with AMR pathogens worldwide, including 1.27 million deaths directly attributable to resistant infections [1]. Projections suggest that, without effective intervention, AMR could result in up to 10 million deaths annually by 2050 [2]. In the United States alone, over 2.8 million AMR infections occur each year, leading to more than 35,000 deaths and imposing an economic burden of approximately $20-35 billion [3].
Recognizing the limitations of traditional practice guidelines in rapidly evolving areas such as AMR, the Infectious Diseases Society of America (IDSA) has developed narrowly focused guidance documents, including on the treatment of AMR infections. This AMR Treatment Guidance document is meant to address important clinical questions where high-quality evidence may be limited or emerging. Developed by a small panel of infectious diseases experts, it is informed by a comprehensive (though not necessarily systematic) review of the literature, combined with clinical expertise and consensus opinion.
This document provides suggestions on the treatment of infections caused by extended-spectrum β-lactamase-producing Enterobacterales (ESBL-E), AmpC β-lactamase-producing Enterobacterales (AmpC-E), carbapenem-resistant Enterobacterales (CRE), Pseudomonas aeruginosa with difficult-to-treat resistance (DTR P. aeruginosa), carbapenem-resistant Acinetobacter baumannii (CRAB), and Stenotrophomonas maltophilia. These pathogens are responsible for a broad spectrum of infections encountered in hospitals across the United States and are associated with substantial morbidity and mortality [4].
Management suggestions are presented in a question-and-answer format for each pathogen. In general, preferred and alternative antibiotic options are listed in alphabetical order in the “suggested approach” sections and more nuance regarding the ranking of agents amongst the preferred and alternative options is provided in the “rationale” sections. While concise summaries of relevant clinical trials, resistance mechanisms, and antimicrobial susceptibility testing (AST) considerations are included, this document is not intended to serve as a comprehensive review of these topics. Furthermore, GRADE methodology (Grading of Recommendations, Assessment, Development, and Evaluation) is not employed. Given international variability in resistance mechanisms and antibiotic availability, treatment suggestions are specific to the United States context. This guidance applies to both adult and pediatric populations. Suggested adult antibiotic dosing for patients with normal renal and hepatic function is summarized in Table 1; pediatric dosing suggestions for select antibiotic agents are available elsewhere [5]. Clinical and Laboratory Standards Institute (CLSI) susceptibility criteria are displayed in Table 2. This document reflects the evidence and expert consensus as of March 1, 2026.
General Management Suggestions
The management suggestions outlined in this guidance assume identification of the causative pathogen and confirmation of in vitro susceptibility to the proposed agents. When multiple antibiotics demonstrate comparable efficacy, selection should also be informed by factors such as safety and tolerability profile, cost and third-party payer coverage, ease of administration, and institutional formulary availability.
Empiric Therapy
While empiric treatment suggestions are beyond the scope of this guidance, initial antibiotic selection should be informed by the most likely pathogens, the severity of illness, the suspected source of infection, and relevant patient-specific factors (e.g., history of severe β-lactam allergy, profound immunosuppression, underlying renal disease). Additional considerations that should inform empiric therapy include: (1) prior microbiologic data, including organisms and associated AST results within the past 12 months; (2) antibiotic exposure in the preceding 3 months; and (3) local epidemiology and cumulative AST data for the most probable pathogens [6-8]. Empiric regimens should be reassessed and refined once the pathogen has been identified, incorporating AST data and the presence of clinically relevant β-lactamases, when available.
Distinguishing infection from colonization remains essential for all pathogens, as inappropriate antibiotic use promotes AMR and places patients at risk for unnecessary harm [9, 10]. Notably, commonly selected empiric regimens often lack activity against CRAB and S. maltophilia. Decisions to include agents targeting these organisms should be individualized and based on a careful assessment of prior culture results, host-specific risk factors, clinical presentation, and the potential for antibiotic-related toxicity.
Duration of Therapy and Transitioning to Oral Therapy
This document does not provide specific suggestions regarding duration of therapy. However, clinicians are advised that treatment durations for infections caused by AMR pathogens generally need not differ from those caused by more susceptible pathogens [11]. Once AST results become available, they may reveal that the empirically selected regimen lacked in vitro activity against the causative organism. This information may influence treatment duration decisions.
For example, uncomplicated urinary tract infections (uUTIs; defined as UTIs confined to the bladder in afebrile women or men) are typically mild and self-limited [12]. If an empiric regimen lacked activity against the uropathogen, but the patient nonetheless exhibited clinical improvement, it is generally not necessary to repeat urine cultures, modify the regimen, or extend the planned treatment course. In contrast, for other infection types, including complicated UTIs (cUTIs), if AST results indicate that the empiric therapy is inactive, a switch to an agent to which the pathogen tested susceptible is suggested, and the treatment duration should be counted from the initiation of active therapy. Of note, a cUTI is defined as an infection of the urinary tract that extends beyond the bladder and includes conditions such as pyelonephritis, febrile or bacteremic UTI, catheter-associated UTI, or prostatitis[12].
As with all infections, host-specific factors - including immune status, adequacy of source control, and clinical response to therapy - should be considered when determining treatment duration. Finally, when feasible, transitioning from intravenous (IV) to oral therapy should be pursued, provided the following criteria are met: (1) the pathogen is susceptible to an appropriate oral agent; (2) the patient is hemodynamically stable; (3) an oral agent anticipated to concentrate at the site of infection is available; and (4) gastrointestinal absorption is expected to be sufficient[13].
Table 1: Antibiotic Dosing Suggestions
Table 1. Suggested Dosing of Antibiotics for the Treatment of Antimicrobial-Resistant Infections in Adults, Assuming Normal Renal and Hepatic Function1-4
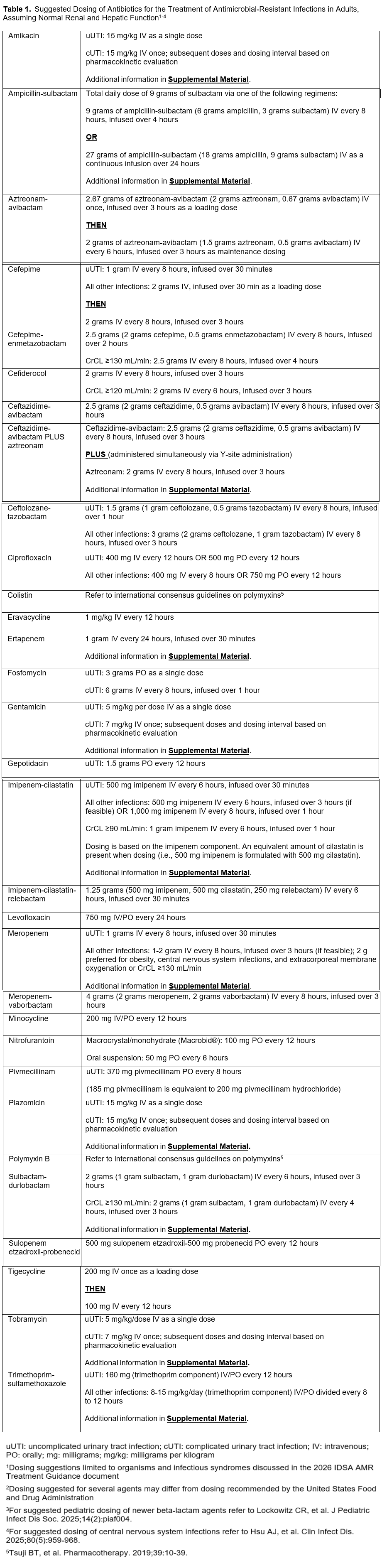
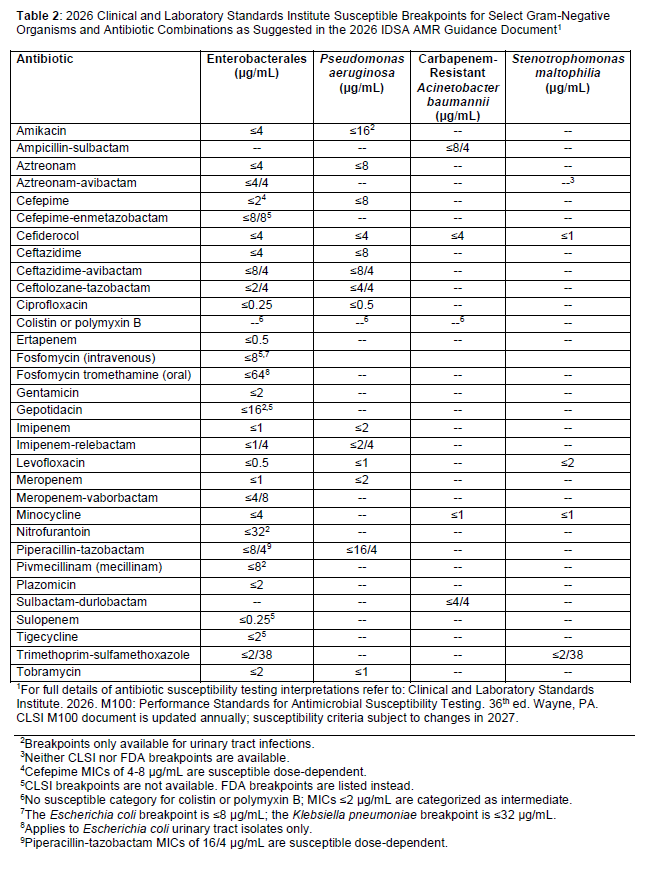
Table 2: Antibiotic Breakpoints
Table 2. 2026 Clinical and Laboratory Standards Institute Susceptible Breakpoints for Select Gram-Negative Organisms and Antibiotic Combinations as Suggested in the 2026 IDSA AMR Guidance Document1
Section 1: Extended-spectrum β-lactamase-Producing Enterobacterales (ESBL-E)
ESBLs are enzymes that inactivate most penicillins, cephalosporins, and aztreonam. ESBL-E generally remain susceptible to carbapenems. ESBLs do not inactivate non-β-lactam agents (e.g., ciprofloxacin, trimethoprim-sulfamethoxazole [TMP-SMX], gentamicin, doxycycline). However, organisms carrying ESBL genes often harbor additional genes or mutations in genes expanding their resistance to a broad range of antibiotics.
Any gram-negative organism has the potential to carry ESBL genes; however, they are most prevalent in Escherichia coli, Klebsiella pneumoniae, and Klebsiella oxytoca [14-16]. CTX-M enzymes, particularly CTX-M-15, are the most common ESBLs in the United States[15]. ESBLs other than CTX-M enzymes with unique hydrolyzing abilities are also present, including variants of TEM and SHV β-lactamases with amino acid substitutions [17-20]. Routine ESBL testing is not performed by most clinical microbiology laboratories and is not considered compulsory by the CLSI [21]. Rather, E. coli, K. pneumoniae, or K. oxytoca isolates resistant to ceftriaxone (i.e., ceftriaxone minimum inhibitory concentrations [MICs] ≥4 µg/mL) is a threshold commonly acknowledged as a surrogate for ESBL-production [15, 22-24]. Treatment suggestions for ESBL-E infections assume that in vitro activity of preferred and alternative antibiotics has been demonstrated.
Question 1.1: What are preferred antibiotics for the treatment of uncomplicated cystitis caused by ESBL-E?
Suggested approach: Aminoglycosides (as a single dose), gepotidacin, nitrofurantoin, pivmecillinam, sulopenem, and TMP-SMX (listed alphabetically and in no preferential order) are preferred treatment options for uUTIs caused by ESBL-E. Oral fosfomycin is an alternative option for uUTIs caused by ESBL-producing E. coli. When resistance, availability, or intolerance preclude the use of preferred or alternative agents, fluoroquinolones (e.g., ciprofloxacin, levofloxacin), cefepime–enmetazobactam, or carbapenems (e.g., ertapenem, meropenem, imipenem) may be used.
Rationale
Because treatment courses for uUTI are brief and access to susceptibility testing, particularly for newer agents, remains limited, therapy for uUTI is often initiated (and completed) before ESBL production is known and in the absence of susceptibility data. This underscores the importance of reviewing prior urine culture results from individual patients and understanding local ESBL-E epidemiology to determine if ESBL-E coverage may be warranted. The prevalence of ESBL-producing E. coli among UTIs in the United States is increasing and estimated at approximately 17%, with substantial regional variability[25]. Of note, for several preferred and alternative agents for the treatment of ESBL-E uUTI, surveillance data indicate that susceptibility exceeds 90% making them reasonable for empiric use in the absence of confirmatory susceptibility data.
Aminoglycosides are nearly exclusively eliminated by the renal route. A systematic review of 13 studies including 13,804 patients demonstrated a pooled microbiologic cure of approximately 95% with single-dose aminoglycoside therapy, with no recurrences in 73% of patients by day 30 [26]. This was further supported by an observational study of 13 patients receiving single-dose aminoglycoside therapy [27]. Although robust clinical trial data are lacking, given the relatively high likelihood of treatment success and low likelihood of nephrotoxicity with single dose treatment, the panelists consider single-dose aminoglycoside therapy a preferred approach for the treatment of ESBL-E uUTI.
Gepotidacin, the first triazaacenaphthylene antibiotic, was approved in March 2025 for the treatment of uUTI. It is an oral antibiotic that inhibits bacterial DNA replication via unique binding sites on DNA gyrase and topoisomerase IV, such that single target-specific mutations that may cause resistance to agents such as ciprofloxacin or levofloxacin do not confer resistance to gepotidacin[28]. Gepotidacin demonstrates activity against more than 90% of ESBL-E isolates[29, 30]. In two randomized clinical trials comparing five days each of gepotidacin and nitrofurantoin, treatment success among the subgroup of women with ESBL-producing E. coli uUTI was numerically more favorable for gepotidacin (70% [35/50] versus 63% [25/40] in one trial; 68% [23/34] versus 40% [10/25] in the second trial [31]). Collectively, these data suggest gepotidacin is at least as effective as another preferred agent for the treatment of ESBL-E uUTI. The most common adverse event with gepotidacin is mild to moderate diarrhea [31, 32]. Given gepotidacin’s activity against Neisseria gonorrhoeae, clinicians should remain cognizant that excessive use could potentially contribute to the selection of resistant N. gonorrhoeae strains[33].
Nitrofurantoin retains high activity against ESBL-E, with susceptibility generally exceeding 90% [34-36]. It is well tolerated, with mild gastrointestinal symptoms being the most common adverse event. In a randomized trial, a 5-day course of nitrofurantoin resulted in significantly higher treatment success than single-dose oral fosfomycin among patients with E. coli uUTI (70% [171/244] versus 58% [139/241])[37]. Although ESBL status was not specified, these findings are likely also applicable to ESBL-E uUTI.
Pivmecillinam, an oral penicillin and prodrug of mecillinam that has been used internationally for decades, was approved in the United States in April 2024. Its distinctive structure renders it a poor substrate for most β-lactamases [38]. Pivmecillinam demonstrates activity against over 90% of ESBL-E isolates [39, 40]. Three-day regimens achieve treatment success in approximately 75-95% of women with uUTI [41, 42]. While observational studies suggest increased failure risk for ESBL-E compared with non-ESBL-E uUTIs, this difference has not been observed with higher dosing (400 mg three times daily) [43]. Pivmecillinam is associated with a favorable safety profile, most commonly mild gastrointestinal adverse events[44]. Its narrow spectrum and low propensity for resistance emergence support its role as a preferred agent. Suggested dosing for pivmecillinam, which differs from the FDA-approved label, is provided in Table 1.
Sulopenem, administered as the oral prodrug formulation sulopenem etzadroxil, which is coformulated with probenecid, is a novel thiopenem antibiotic that achieved FDA-approval in October 2024. It is active against over 95% of ESBL-E isolates [45]. When administered for 5 days for uUTI, sulopenem had similar treatment success (i.e., overall clinical and microbiological response) as a 3-day course of ciprofloxacin for patients with ESBL-E uUTIs (56% [41/73] versus 47% [34/72])[46]. Mild diarrhea is the most common adverse event associated with sulopenem. Notably, probenecid inhibits tubular secretion and may increase plasma concentrations of other drugs (e.g. methotrexate, piperacillin, sulfonamides) [47].
TMP-SMX, as a three-day course, is effective for ESBL-E uUTI when the infecting isolate is susceptible, with clinical efficacy comparable to three-day courses of fluoroquinolones [48]. However, susceptibility among ESBL-E urinary isolates in the United States is limited to approximately 50% [49], necessitating close clinical monitoring when used empirically. Short-course therapy is generally well tolerated, though nausea, emesis, and hypersensitivity reactions may occur [50].
Oral fosfomycin as a single dose is an alternative option for uUTI caused by ESBL-producing E. coli. Although E. coli susceptibility to fosfomycin is not routinely assessed in clinical microbiology laboratories, resistance remains uncommon in the United States [51]. Oral fosfomycin is not suggested for gram-negative organisms other than E. coli because of the high prevalence of fosA genes, including K. pneumoniae, which may enzymatically inactivate fosfomycin and compromise clinical efficacy [52-54]. Admittedly, clinical outcome studies investigating the clinical impact of fosA are not available. In a randomized trial, single-dose oral fosfomycin was associated with lower clinical success than a 5-day course of nitrofurantoin among E. coli uUTI (58% [139/241] versus 70% [171/244])[37]. Mild diarrhea is the most common adverse event associated with oral fosfomycin [55]. The clinical benefit of multidose oral fosfomycin for uUTI remains uncertain but may be a reasonable consideration, extrapolating from data in cUTI[56] (Question 1.2). The role of IV fosfomycin for cUTI is also discussed in Question 1.2.
Amoxicillin-clavulanic acid is not suggested for the treatment of ESBL-E uUTI. A randomized clinical trial compared three-day regimens of amoxicillin-clavulanic acid (500 mg/125 mg twice daily) to ciprofloxacin (250 mg twice daily) for 370 women with E. coli uUTI [57]. Clinical cure was observed in 58% (93/160) and 77% (124/162) of the women randomized to the amoxicillin-clavulanic acid and ciprofloxacin arms, respectively. The higher failure with amoxicillin-clavulanic acid may be associated with persistent vaginal bacterial colonization, which occurred in 45% (68/151) and 10% (16/153) of patients in the amoxicillin-clavulanic acid and ciprofloxacin arms, respectively. The proportion of women in the trial infected with ESBL-E isolates is not available. Of note, both agents were administered at dosages lower than suggested (Table 1). Even though clavulanic acid inhibits ESBL enzymes in vitro [58, 59], this may not translate to clinical efficacy, particularly when extrapolating from studies evaluating the efficacy of amoxicillin-clavulanic acid for uUTI, independent of resistance phenotype [57, 60].
The panel suggests avoiding doxycycline for ESBL-E uUTI given its relatively low urinary concentrations, with only 35-60% excreted unchanged in urine[61]. Limited clinical data supporting its use for UTI derive from small studies that primarily involved P. aeruginosa, an organism resistant to oral tetracyclines, thereby limiting their interpretability [62, 63].
Although cefepime-enmetazobactam, fluoroquinolones (e.g., ciprofloxacin, levofloxacin) – if susceptibility has been demonstrated, and carbapenems (e.g., ertapenem, meropenem, imipenem-cilastatin; henceforth, imipenem) are typically effective against ESBL-E uUTI (Question 1.2), the panel suggests reserving these agents for cUTI and other invasive ESBL-E infections, given the availability of multiple effective alternatives for uUTI. Traditional β-lactams (e.g., piperacillin-tazobactam, cefepime, cephamycins) are likewise not designated as preferred options for ESBL-E uUTI; considerations regarding continuation of these agents when empirically initiated for uUTI are addressed in Question 1.4, Question 1.5, and Question 1.6, respectively.
Question 1.2: What are preferred antibiotics for the treatment of cUTI caused by ESBL-E?
Suggested approach: TMP-SMX, ciprofloxacin, or levofloxacin are preferred agents for the treatment of cUTI caused by ESBL-E, when in vitro susceptibility is demonstrated. Cefepime-enmetazobactam, or carbapenems (ertapenem, meropenem, or imipenem) are preferred when resistance, intolerance, or toxicities preclude use of TMP-SMX or fluoroquinolones. IV fosfomycin, aminoglycosides, and piperacillin-tazobactam, are alternative options for ESBL-E cUTI.
Rationale
TMP-SMX, ciprofloxacin, and levofloxacin are preferred treatment options for ESBL-E cUTI when susceptibility is confirmed, based on their ability to achieve sustained urinary concentrations, supportive clinical trial data, and extensive clinical experience [64-66]. When IV therapy is initiated and susceptibility to TMP-SMX, ciprofloxacin, or levofloxacin is demonstrated, transition to one of these oral agents is preferred.
Cefepime-enmetazobactam or carbapenems are preferred when oral TMP-SMX or fluoroquinolones cannot be administered (Question 1.3). Surveillance data indicate that enmetazobactam restores cefepime’s activity against almost all ESBL-E isolates [67]. In a randomized trial of cUTI, treatment success was observed in 74% (56/76) of patients receiving cefepime-enmetazobactam for infections due to ESBL-E, compared with 52% (34/66) for those receiving piperacillin-tazobactam [68]. In the absence of direct comparisons between cefepime-enmetazobactam and carbapenems for the treatment of ESBL-E cUTI, the panel considers both to be equally effective options.
IV fosfomycin, approved by the FDA in October 2025, is an alternative treatment for ESBL-E cUTIs. In a randomized clinical trial, amongst 111 patients with ESBL-E cUTI, 7 days of IV fosfomycin and piperacillin-tazobactam were associated with clinical cure in 93% (52/56) and 93% (51/55) of patients, respectively [69]. In a randomized open-label that included 81 patients with presumed ESBL-E. coli cUTI and bacteremia, clinical and microbiological cure occurred in 59% (23/39) of patients receiving IV fosfomycin and 71% (30/42) of those receiving meropenem [70]. Although this difference was not statistically significant, fosfomycin did not achieve non-inferiority to comparator agents in the overall trial. Additional clinical data are needed before considering IV fosfomycin as a preferred therapy. The sodium content of IV fosfomycin exceeds recommended daily intake and warrants caution in older adults and patients at risk for heart failure [71]. The panel suggests IV fosfomycin as an alternative treatment option for cUTIs caused by E. coli. FDA susceptibility criteria exist for IV fosfomycin against K. pneumoniae, in contrast to oral fosfomycin (Table 2). However, K. pneumoniae frequently harbors fosA, which may inactivate fosfomycin [52-54]. Reassuringly, in a subgroup analysis of a clinical trial including patients with K. pneumoniae cUTI, clinical cure was achieved in 93% (25/27) and 100% (25/25) of patients randomized to 7 days of IV fosfomycin or piperacillin-tazobactam, respectively[69]. Pending additional supportive clinical data, the panel advises careful consideration when prescribing IV fosfomycin for ESBL-producing K. pneumoniae infections.
Aminoglycosides are alternative options for ESBL-E cUTI. Although expected to be effective as they achieve high renal parenchymal concentrations [72], duration-dependent nephrotoxicity should be carefully considered [73, 74]. In a randomized clinical trial of 609 patients with cUTI (28% caused by ESBL-E), clinical cure occurred in 89% (170/191) and 90% (178/197) of patients receiving plazomicin and meropenem, respectively[75]. Acute kidney injury occurred in 7% (21/300) of patients receiving plazomicin compared with 4% (12/297) receiving meropenem. Among patients with ESBL-E cUTI, microbiological eradication was achieved in 82% (42/51) and 75% (45/60) of patients, respectively. Other aminoglycosides are likely equally effective if susceptibility is demonstrated [76-78]. A randomized clinical trial of 61 patients with cUTI (including 40 with ESBL-E cUTI) demonstrated similar clinical cure between those receiving three doses of amikacin 1g every 48 hours versus meropenem for 7 days[76]. Aminoglycosides may be reasonable to consider for completing treatment courses (e.g., transitioning from another agent for terminal doses) given their prolonged duration of activity in the renal cortex and the convenience of once daily dosing[77, 79]. The role of piperacillin-tazobactam as an alternative treatment for cUTI is summarized in Question 1.4.
In a randomized trial investigating sulopenem for the treatment of cUTI, both arms received 5 initial days of IV therapy (i.e., sulopenem or ertapenem) prior to transitioning to oral therapy[80]. Sulopenem did not achieve noninferiority for the primary endpoint of combined clinical and microbiologic response at day 21 (68% [301/444] versus 74% [325/440]). Clinical success, however, was similar (89% [397/444] versus 88% [389/440]), as was overall favorable response among patients with ESBL-positive infections (72% [79/110] versus 68% [85/125]). Given the inclusion of 5 initial days of IV sulopenem in this trial, oral sulopenem is suggested as an alternative option for ESBL-E cUTI only after initial clinical improvement has been observed. Notably, IV sulopenem is not currently FDA-approved for clinical use.
Although oral fosfomycin is not suggested as initial therapy for cUTI because of limited renal parenchymal concentrations, it may be considered for transition therapy in select circumstances for ESBL-E. coli cUTI when other oral options are unavailable. Clinical trials evaluating multidose oral fosfomycin following short courses of IV therapy demonstrated similar clinical cure compared with fluoroquinolones; however, ESBL-E representation was limited, and IV treatment durations prior to initiation of oral fosfomycin often approximated the total duration typically required for cUTI[56, 81]. Further data are needed before oral fosfomycin can be considered a preferred option for transition therapy for cUTIs.
Question 1.3: What are preferred antibiotics for the treatment of infections outside of the urinary tract caused by ESBL-E?
Suggested approach: Ertapenem, imipenem, and meropenem are preferred agents for the treatment of ESBL-E infections outside of the urinary tract. Imipenem or meropenem are preferred for patients who are critically ill or those with hypoalbuminemia. Cefepime-enmetazobactam is an alternative option for ESBL-E infections outside of the urinary tract. Once an appropriate clinical response has been achieved, transition to oral ciprofloxacin, levofloxacin, or TMP-SMX may be considered, provided in vitro susceptibility is demonstrated.
Rationale
Carbapenems are a preferred treatment for invasive ESBL-E infections based on an open-label clinical trial that enrolled 391 patients with ESBL-E bloodstream infections (86% with confirmed ESBL genes) [82]. Patients were randomized to receive either piperacillin-tazobactam 4.5 grams IV every six hours or meropenem 1 grams IV every eight hours, administered as 30-minute infusions. 30-day survival occurred in 88% (164/187) of patients in the piperacillin-tazobactam arm compared with 96% (184/191) in the meropenem arm. These trial data were subsequently reanalyzed to include only patients with clinical isolates for which piperacillin-tazobactam MICs were ≤16 µg/mL as determined by broth microdilution, the reference standard for AST [22]. Among the 320 patients (82%) with isolates available for retesting, 30-day survival occurred in 91% (134/147) of patients receiving piperacillin-tazobactam and 96% (149/155) of those receiving meropenem. Although the absolute risk difference was attenuated and no longer statistically significant in the reanalysis (95% confidence interval, −1% to 11%) [22], the panel continues to favor carbapenem therapy as the preferred treatment for ESBL-producing bloodstream infections given the consistent direction of the mortality difference overall and across individual subgroup analyses. Additional limitations of piperacillin-tazobactam that suggest caution with its administration for invasive infections due to ESBL-E are discussed in Question 1.4. The panel further suggests extrapolating evidence from ESBL-E bloodstream infections to other common sites of infection, including intra-abdominal infections, skin and soft tissue infections, and pneumonia.
For patients who are critically ill and/or have hypoalbuminemia, imipenem or meropenem are preferred over ertapenem. In contrast to imipenem and meropenem, ertapenem is highly protein bound, resulting in a prolonged serum half-life[83]. In patients with hypoalbuminemia, the unbound fraction of ertapenem increases, leading to enhanced clearance and a shortened serum half-life [83-86]. In an observational study of 279 patients with Enterobacterales infections, hypoalbuminemia (defined as serum albumin <2.5 g/dL) was associated with a higher odds of 30-day mortality among patients treated with ertapenem compared with those receiving imipenem or meropenem[87].
Clinical data comparing ertapenem with other carbapenems in critically ill patients are limited and conflicting [85, 88]. However, given concerns regarding variable and unpredictable interpatient pharmacokinetics [85, 89], the panel suggests meropenem or imipenem rather than ertapenem as initial therapy for critically ill patients with ESBL-E infections. Although higher doses of ertapenem (e.g., 1.5 g daily) or more frequent dosing (e.g., every 12 hours) may mitigate some probability-of-target-attainment concerns in obese or critically ill patients and those with hypoalbuminemia, data demonstrating improved outcomes with these alternative dosing strategies are limited [89-91].
Cefepime-enmetazobactam represents an alternative for the treatment of ESBL-E infections outside the urinary tract. This suggestion is supported by extensive clinical experience with cefepime for invasive infections; particularly when administered at high doses via extended infusion, combined with the inhibitory activity of enmetazobactam against ESBLs [67], and pharmacokinetic/pharmacodynamic (PK/PD) modeling demonstrating adequate intrapulmonary penetration and a high probability of target attainment for both agents against Enterobacterales isolates with MICs ≤8/8 µg/mL [92]. Compared with tazobactam, enmetazobactam contains a methyl substitution that confers a net neutral charge and zwitterionic structure, enhancing bacterial cell penetration and increasing periplasmic concentrations, thereby complementing cefepime’s zwitterionic oxyimino-cephalosporin activity[93]. Clinical data evaluating cefepime-enmetazobactam for ESBL-E infections outside the urinary tract remain limited. Although its pharmacologic properties suggest expected efficacy for invasive ESBL-E infections, additional evidence is needed before it can be suggested as a preferred therapy.
Given the high oral bioavailability and sustained serum exposures achieved with oral TMP-SMX and fluoroquinolones, transition to these agents should be considered for patients with ESBL-E infections when all of the following criteria are met: (1) in vitro susceptibility to the selected agent is confirmed, (2) the patient is hemodynamically stable, and (3) there are no concerns regarding impaired gastrointestinal absorption. In contrast, oral step-down therapy with nitrofurantoin, fosfomycin, amoxicillin-clavulanate, omadacycline, or doxycycline are not suggested for ESBL-E bloodstream infections due to concerns with achieving adequate serum concentrations and/or limited clinical data supporting their efficacy for ESBL-E bacteremia.
Until more PK/PD analyses and clinical data is available, the use of oral sulopenem as transition therapy for ESBL-E bloodstream infections is not suggested. In a subgroup analysis of 77 patients with cUTI and associated bacteremia enrolled in a randomized clinical trial, treatment success occurred in 57% (25/44) and 65% (28/43) of those transitioned to oral sulopenem (from IV sulopenem) and oral ciprofloxacin or amoxicillin-clavulanate (from IV ertapenem), respectively[80]. In a randomized clinical trial of patients with intra-abdominal infections, clinical success was 82% (204/249) for sulopenem-treated patients (i.e., 5 days of IV sulopenem followed by oral sulopenem) versus 88% (233/265) in the alternative arm (i.e., 5 days of IV ertapenem followed by oral ciprofloxacin/metronidazole or amoxicillin-clavulanate) [94].
Question 1.4: Is there a role for piperacillin-tazobactam in the treatment of infections caused by ESBL-E?
Suggested approach: If piperacillin-tazobactam is initiated as empiric therapy for an uUTI caused by an organism subsequently identified as an ESBL-E and the patient demonstrates clinical improvement, neither a change in therapy nor an extension of treatment duration is necessary. The panel suggests piperacillin-tazobactam as an alternative treatment option for cUTI caused by ESBL-E in patients who are not critically ill and who do not have concomitant bacteremia. In contrast, piperacillin-tazobactam is not suggested for the treatment of ESBL-E infections at sites outside of the urinary tract, even when in vitro susceptibility to piperacillin-tazobactam is demonstrated.
Rationale
Piperacillin-tazobactam often demonstrates in vitro activity against ESBL-E[95]. However, there are several concerns regarding tazobactam’s ability to function as an effective β-lactamase inhibitor for ESBL-E. First, piperacillin-tazobactam MIC testing may be inaccurate and/or poorly reproducible when ESBL enzymes are present, or in the presence of other β-lactamase enzymes such as OXA-1, making it unclear if an isolate that tests susceptible to this agent is reliably susceptible [22, 96-98]. Second, preclinical data indicate that with increased bacterial inoculum which may be present in certain clinical infections (e.g., abscesses), regrowth of ESBL-E isolates is more likely with piperacillin-tazobactam than with meropenem, although the clinical implications of these findings are unclear[99-101]. Third, the effectiveness of tazobactam may be diminished for organisms with increased expression of ESBL enzymes or by the presence of multiple ESBL or other β-lactamases (e.g., AmpC enzymes)[93]. This may in part be due to the low concentration of tazobactam relative to the amount of piperacillin [102]. More specifically, in a 4.5-gram dose of piperacillin-tazobactam there is an 8:1 ratio of piperacillin to tazobactam (i.e., 4 grams of piperacillin and 0.5 grams of tazobactam). In contrast, in a 3-gram dose of ceftolozane-tazobactam there is a 2:1 ratio of ceftolozane to tazobactam. Finally, the piperacillin-tazobactam breakpoint for Enterobacterales is primarily based on PK/PD considerations of piperacillin dosing strategies and not on whether a fixed concentration of 4 µg/mL of tazobactam in testing wells is reflective of the restorative ability of commonly prescribed tazobactam dosages to reestablish the activity of piperacillin in infections with ESBL-production.
If piperacillin-tazobactam was initiated as empiric therapy for uUTI caused by an organism later identified as an ESBL-E and clinical improvement occurs, no change or extension of antibiotic therapy is necessary, given the high urinary concentration of piperacillin-tazobactam[103].
Piperacillin–tazobactam is an alternative treatment for cUTI caused by ESBL-E. A systematic review of one randomized clinical trial[104] and six observational studies including 1,156 patients treated with either piperacillin–tazobactam or carbapenems for ESBL-E UTIs found comparable treatment success between the regimens[105]. The included clinical trial of 66 patients with ESBL-E cUTI demonstrated similar treatment success with piperacillin–tazobactam and ertapenem, at 94% (31/33) and 97% (32/33), respectively[104]. In a separate randomized clinical trial involving 111 patients with ESBL-E cUTI, IV fosfomycin and piperacillin–tazobactam were associated with 93% (52/56) and 93% (51/55) clinical cure [69]. However, among the subgroup of 231 patients with ESBL-E bloodstream infections originating from the urinary tract enrolled in a clinical trial comparing piperacillin-tazobactam with meropenem, survival was numerically lower in the piperacillin-tazobactam arm (93% [95/102] versus 97% [124/128]) [82]. The panel does not suggest piperacillin–tazobactam for the treatment of ESBL-E cUTI in patients who are critically ill or with concomitant bacteremia.
Piperacillin-tazobactam is also not suggested for the treatment of invasive ESBL-E infections based on the results of the aforementioned clinical trial which indicated inferior results with piperacillin-tazobactam compared to carbapenem therapy[82]. A second trial investigating the role of piperacillin-tazobactam for the treatment of ESBL-E bloodstream infections is ongoing[106]. A 2023 meta-analysis including 2,786 patients across the clinical trial [82] and 25 observational studies found no difference in survival between β-lactam/β-lactamase inhibitors (not limited to piperacillin-tazobactam) and carbapenems [107]. Two subsequent observational studies, one including 644 patients[108] and another including 264 patients[109] had conflicting findings with one suggesting no difference in survival (92% [283/309] versus 92% [308/335]) [108] and the second indicating lower survival in the empiric piperacillin-tazobactam group (86% [172/200] versus 96% [61/64]) [109]. Given the concerns with pre-clinical data for piperacillin-tazobactam against higher burden infections and clinical trial results indicating suboptimal outcomes with piperacillin-tazobactam for ESBL-E bloodstream infections, piperacillin-tazobactam is not suggested as a preferred or alternative treatment for ESBL-E invasive infections.
Question 1.5: Is there a role for cefepime in the treatment of infections caused by ESBL-E?
Suggested approach: If cefepime was initiated as empiric therapy for uUTI caused by an organism later identified as an ESBL-E and clinical improvement occurs, no change or extension of antibiotic therapy is necessary. The panel suggests avoiding cefepime for the treatment of cUTI or infections outside of the urinary tract caused by ESBL-E, even if susceptibility to cefepime is demonstrated.
Rationale
ESBLs commonly hydrolyze cefepime[93, 110, 111] in the absence of protection with a β-lactamase inhibitor (e.g., enmetazobactam). Furthermore, even if ESBL-producing isolates test susceptible to cefepime, cefepime MIC testing may be inaccurate and/or poorly reproducible with commercial AST methods[112]. Clinical trials comparing the outcomes of patients with ESBL-E bloodstream infections treated with cefepime or carbapenems have not been conducted.
If cefepime was initiated as empiric therapy for uUTI caused by an organism later identified as an ESBL-E and clinical improvement occurs, no change or extension of antibiotic therapy is necessary, given the high urinary concentration of cefepime[113].
Although some observational studies evaluating the role of cefepime versus carbapenems for ESBL-E cUTI suggest no difference in clinical outcomes[114, 115], in a clinical trial of ESBL-E cUTI the cefepime arm was terminated early because of a clinical failure signal with cefepime (2 grams IV every 12 hours), despite all isolates having cefepime MICs of 1-2 µg/mL; with clinical success in 33% (2/6) and 97% (32/33) of patients receiving cefepime and ertapenem, respectively [104]. The panel suggests avoiding cefepime for the treatment of ESBL-E cUTI.
Observational studies comparing cefepime and carbapenems for the treatment of invasive ESBL-E infections demonstrated either no difference in outcomes or poorer outcomes with cefepime [116-120]. Clinical trials comparing cefepime to carbapenems for ESBL-E bloodstream infections have not been conducted. However, a subgroup analysis of patients with ESBL-E pneumonia enrolled in a clinical trial identified clinical success in 69% (9/13) versus 100% (10/10) of patients randomized to cefepime (2 g IV every 8 hours) and imipenem (500 mg IV every 6 hours), respectively [121]. The panel suggests avoiding cefepime for the treatment of invasive ESBL-E infections.
Question 1.6: Is there a role for the cephamycins in the treatment of infections caused by ESBL-E?
Suggested approach: Cephamycins are not suggested for the treatment of ESBL-E infections until more clinical outcomes data using cefoxitin or cefotetan are available and optimal dosing has been defined.
Rationale
Cephamycins are a subclass of cephalosporins that are generally stable against hydrolysis by ESBL enzymes [122, 123]. In the United States, cefoxitin and cefotetan are the only available cephamycins; both are administered IV. At least 10 observational studies have compared clinical outcomes of patients with ESBL-E infections treated with cephamycins versus carbapenems, most commonly UTIs or bloodstream infections from urinary sources [124-130]. Eight of these studies reported no differences in clinical outcomes, whereas two demonstrated poorer outcomes with cephamycins [125, 130] – including the largest study which identified 30-day survival of 71% (94/132) versus 87% (115/132) for cephamycins and carbapenems, respectively, amongst patients with ESBL-E bacteremia [130]. Interpretation of these studies is limited by the observational design of all studies, heterogeneity in infection sources, substantial selection bias, and variability in cephamycin agents, dosing strategies, and durations of therapy.
Although not available for clinical use in the United States, the most encouraging data supporting the effectiveness of cephamycins against ESBL-E are for cefmetazole [128, 129, 131, 132], which is being compared to meropenem in a clinical trial of patients with ESBL-E bacteremia [133].
Many cephamycins evaluated in published studies are not available in the United States, and relatively few patients have received cefoxitin or cefotetan in clinical investigations [127, 134, 135]. Additional clinical data, including optimized dosing and administration strategies, are needed before these agents can be endorsed for the treatment of ESBL-E infections. While limited data suggest improved outcomes with high-dose, continuous-infusion cefoxitin (e.g., 6 g daily)[134, 135], the IV-only formulation and relatively short half-lives of both agents, particularly cefoxitin, offer no clear feasibility or clinical advantage over preferred agents for the treatment of ESBL-E infections. Based on available data, the panel does not suggest cephamycins for the treatment of ESBL-E infections.
Question 1.7: What is the role of β-lactam agents with activity against carbapenem-resistant organisms for the treatment of infections caused by ESBL-E?
Suggested approach: While effective against ESBL-E infections, the panel suggests that aztreonam-avibactam, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-relebactam, ceftolozane-tazobactam, and cefiderocol be preferentially reserved for treating infections caused by organisms exhibiting carbapenem resistance.
Rationale
Aztreonam-avibactam, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam (henceforth, imipenem-relebactam), ceftolozane-tazobactam, and cefiderocol exhibit activity against ESBL-E [45, 136]. Avibactam can successfully protect aztreonam and ceftazidime against hydrolysis by ESBL enzymes [15, 137]. Subgroup analysis of clinical trial data support ceftazidime-avibactam’s effectiveness against ESBL-E infections [138-142]. The carbapenem component of meropenem-vaborbactam and imipenem-relebactam provide sufficient activity against ESBL-E, even without the addition of a β-lactamase inhibitor.
Ceftolozane-tazobactam is more potent against ESBL-E than piperacillin-tazobactam, with the addition of tazobactam leading to ceftolozane MICs that are several dilutions lower than piperacillin MICs [143-148]. Moreover, ceftolozane appears to have greater stability to hydrolysis by common ESBL enzymes (e.g., CTX-M-15) compared to piperacillin, making ceftolozane less reliant than piperacillin on tazobactam's inhibitory properties[149, 150]. Additionally, the ratio of β-lactam to tazobactam present in ceftolozane-tazobactam (2:1) results in greater concentration of tazobactam compared to piperacillin-tazobactam (8:1). In a subgroup analysis of patients with ESBL-E intra-abdominal infections and UTIs from randomized clinical trials, ceftolozane-tazobactam was associated with similar clinical cure as meropenem (97% [76/78] versus 89% [23/26]) [151]. In a subgroup analysis of a clinical trial comparing ceftolozane-tazobactam versus meropenem for ESBL-E pneumonia, 28-day survival was similar between patients receiving ceftolozane-tazobactam (79% [66/84]) and meropenem (71% [52/73]) [152, 153].
Although aztreonam-avibactam, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-relebactam, ceftolozane-tazobactam, and cefiderocol are expected to be effective against ESBL-E infections, the panel suggests that these agents be preferentially reserved for treating carbapenem-resistant organisms or polymicrobial infections with organisms exhibiting carbapenem resistance (e.g., ceftolozane-tazobactam for coinfection with DTR P. aeruginosa and ESBL-E).
Section 2: AmpC β-Lactamase-Producing Enterobacterales (AmpC-E)
AmpC β-lactamases (herein, referred to as AmpC for brevity) are produced at basal levels by several Enterobacterales species, where they play a physiological role in cell wall recycling [154]. These enzymes hydrolyze a range of β-lactams - rendering these agents ineffective - either at basal expression levels (e.g., cefazolin) or, more notably, when AmpC production is increased above basal levels (e.g., ceftriaxone) [155-157]. In Enterobacterales, increased AmpC production arises via three main mechanisms:
- Inducible chromosomal expression of ampC
- Constitutive chromosomal ampC hyperexpression due to mutations in regulatory genes
- Plasmid-mediated ampC genes - which may be integrated into the bacterial chromosome in some species
Inducible expression is triggered by exposure to specific β-lactam agents, leading to significant periplasmic AmpC accumulation sufficient to elevate MICs to agents such as aztreonam, cefotaxime, ceftazidime, ceftriaxone, and piperacillin-tazobactam. Clinically, this can result in an isolate that initially tests ceftriaxone-susceptible becoming resistant during therapy, sometimes after only a few doses of the β-lactam[158]. In this guidance, such organisms are classified as having a moderate risk for clinically significant AmpC production.
In contrast, with constitutive chromosomal ampC hyperexpression or plasmid-mediated ampC, AmpC production remains persistently elevated; isolates typically demonstrate non-susceptibility to cefotaxime, ceftazidime, and ceftriaxone at baseline. Constitutive hyperexpression may arise in certain E. coli or Shigella species through mutations in ampC promoters or attenuators, or in ampC regulatory genes such as ampD, ampR, or ampG. Given the complexity of the ampC regulatory network, the prevalence and functional impact of specific mutations on AmpC overproduction is not well defined[159, 160].
Plasmid-mediated ampC genes (e.g., blaACT, blaCMY, blaDHA, blaFOX, blaMIR) may be carried on plasmids (e.g., blaCMY in E. coli) or integrated into the chromosome (e.g., blaCMY in Citrobacter freundii)[161]. Their prevalence varies geographically. In United States cohorts, plasmid-mediated ampC genes are detected in <10% of ceftriaxone-non-susceptible isolates and are largely confined to E. coli and K. pneumoniae[160, 162]. When present, CMY-type enzymes, particularly CMY-2, predominate in E. coli, whereas both CMY- and DHA-type enzymes are produced by K. pneumoniae [160, 162]. This guidance focuses on the treatment of infections caused by Enterobacterales species with a moderate likelihood of inducible ampC expression, corresponding to the first of the three mechanisms outlined above.
Question 2.1: Which commonly identified Enterobacterales species should be considered at moderate risk for clinically significant inducible ampC production?”
Suggested approach: Enterobacter cloacae complex, Klebsiella aerogenes, and Citrobacter freundii are the most frequently encountered Enterobacterales at moderate risk for clinically significant inducible ampC. Although clinical experience is limited, in vitro data suggest Hafnia alvei exhibits similar inducible ampC potential and may be considered in the same risk category.
Rationale
The optimal method to define the likelihood of clinically significant ampC induction across bacterial species would be to systematically identify organisms that initially test susceptible to select β-lactams (e.g., ceftriaxone) and, following β-lactam exposure, subsequently test resistant - confirmed through genotyping and expression analyses to verify recovery of the same strain and demonstrate increased AmpC production. Such comprehensive studies, however, are not available.
Commonly used mnemonics for AmpC-producing organisms (e.g., SPACE, SPICE, ESCPM) oversimplify the wide spectrum of ampC induction potential among gram-negative bacteria and obscure important interspecies differences. For example, C. freundii carries a chromosomal ampC gene, whereas C. koseri does not [163, 164]. As a result, these acronyms may both underestimate and overestimate the true risk of clinically significant AmpC production. Similarly, “indole-positive Proteus species” have been historically included in such acronyms; however, P. vulgaris, a currently recognized indole-positive species, generally lacks a chromosomal ampC. Common mnemonics previously encompassed P. rettgeri and P. morganii (now Providencia rettgeri and Morganella morganii, respectively)[165], making their continued inclusion in acronyms inaccurate.
The emergence of clinically significant ampC expression during treatment is most frequently documented for E. cloacae complex (hereafter, referred to as E. cloacae), K. aerogenes (formerly Enterobacter aerogenes), and C. freundii. Clinical reports suggest that resistance emergence after exposure to agents such as ceftriaxone may occur in ~20% of infections caused by these organisms[158, 166-168]. These observations are consistent with in vitro data, which also indicate that H. alvei is capable of AmpC overproduction[169, 170]. Accordingly, when E. cloacae, K. aerogenes, C. freundii, or H. alvei are recovered in clinical cultures, the panel suggests generally avoiding cefotaxime, ceftazidime, and ceftriaxone, even if initial AST results indicate susceptibility (Question 2.2). For non-severe infections with adequate source control caused by these species, if one of these agents has been initiated and the patient demonstrates appropriate clinical improvement, completing the treatment course may be reasonable. Regardless of inducibility, basal AmpC production in these organisms confers intrinsic resistance to ampicillin, amoxicillin-clavulanate, ampicillin-sulbactam, first-generation cephalosporins, and cephamycins [21].
By contrast, organisms historically considered at moderate risk for clinically significant ampC derepression - such as Morganella morganii, Providencia spp., and Serratia marcescens, - appear less prone to ampC overexpression, based on both in vitro analyses [169, 171] and clinical observations [158, 166]. Notably, one observational study reported poorer outcomes with ceftriaxone therapy compared to cefepime or carbapenem therapy among patients infected with organisms at lower risk of ampC induction, primarily M. morganii and S. marcescens [172]. However, this association was not replicated in a subsequent observational study [173]. Overall, available evidence suggests that clinically significant AmpC production occurs in fewer than 5% of infections due to these species. Accordingly, when M. morganii, Providencia spp., and S. marcescens are isolated, the panel suggests selecting antibiotic therapy according to AST results, given the lack of data suggesting harm with this approach.
Several less common clinical pathogens (e.g., Citrobacter youngae, Yersinia enterocolitica) harbor inducible chromosomal ampC genes but remain insufficiently studied [169, 174-176]. Consequently, data regarding their propensity for clinically significant AmpC overproduction are limited. For these organisms, it is reasonable to base therapeutic decisions on AST results (e.g., ceftriaxone can be administered if susceptible). However, in the context of infections caused by these less frequently encountered organisms - or by M. morganii, Providencia spp., or S. marcescens - that are characterized by a high bacterial burden and limited source control (e.g., endocarditis, central nervous system infections), consideration of cefepime as an alternative to ceftriaxone is reasonable, even when ceftriaxone susceptibility is demonstrated. As with all infections, if an adequate clinical response is not achieved despite appropriate antibiotic dosing and necessary source-control measures, clinicians should maintain a high index of suspicion for the emergence of resistance to the initially prescribed agent.
Question 2.2: What features should be considered in selecting antibiotics for infections caused by organisms at moderate risk of clinically significant AmpC production due to an inducible ampC gene?
Suggested approach: Several β-lactam antibiotics are at moderate risk for inducing ampC genes. Both the ability to induce ampC genes and the relative stability of the β-lactam agent against hydrolysis by AmpC-E should inform antibiotic decision-making.
Rationale
β-lactam antibiotics fall within a spectrum of potential for inducing ampC genes. Aminopenicillins (i.e., amoxicillin, ampicillin), narrow spectrum (i.e., first-generation) cephalosporins, and cephamycins are potent ampC inducers [177]. However, both organisms at low risk (e.g., S. marcescens) and at moderate risk (e.g., E. cloacae) for clinically significant ampC induction hydrolyze these antibiotics even at basal ampC expression levels. Therefore, AmpC-E isolates, regardless of ampC induction status, will generally test as resistant to these drugs.
Imipenem is also a potent ampC inducer but it generally remains stable to AmpC-E hydrolysis because of the formation of stable acyl enzyme complexes [178]. The induction potential of ertapenem and meropenem has not been formally investigated but, like imipenem, they are generally stable to AmpC hydrolysis [179, 180].
Aztreonam, cefotaxime, ceftazidime, ceftriaxone, and piperacillin-tazobactam are relatively weak ampC inducers [177, 181, 182]. Despite their limited ability to induce ampC, the susceptibility of these agents to hydrolysis makes them less likely to be effective for the treatment of infections by organisms at moderate risk for clinically significant AmpC production [180, 183-186]. They remain, however, reasonable treatment options for Enterobacterales at lower risk for clinically significant AmpC production (e.g., S. marcescens).
Cefepime has the advantage of both being a weak inducer of ampC and of withstanding hydrolysis by AmpC β-lactamases because of the formation of stable acyl enzyme complexes [187-189]. Therefore, cefepime is generally an effective agent for the treatment of AmpC-E infections [190, 191]. TMP-SMX, fluoroquinolones, aminoglycosides, tetracyclines, and other non-β-lactam antibiotics do not induce ampC and are also not substrates for AmpC hydrolysis (Question 2.7).
Question 2.3: What is the role of cefepime for the treatment of infections caused by Enterobacterales at moderate risk of clinically significant AmpC production due to an inducible ampC gene?
Suggested approach: Cefepime is suggested for the treatment of infections caused by organisms at moderate risk of significant AmpC production (i.e., E. cloacae complex, K. aerogenes, C. freundii, H. alvei), if cefepime MICs are in the susceptible or susceptible dose-dependent range (i.e., ≤8 µg/mL).
Rationale
Cefepime, an oxyimino-cephalosporin, demonstrates relative stability against AmpC β-lactamases and exhibits a low propensity for ampC induction [187-189, 192]. Clinical trials comparing cefepime with carbapenems for the treatment of AmpC-E infections have not been conducted. A 2025 meta-analysis encompassing seven studies and 1,099 patients with bacteremia caused by E. cloacae, K. aerogenes, C. freundii, M. morganii, Providencia spp., or S. marcescens found no differences in mortality, clinical cure, or infection relapse between cefepime and carbapenem recipients [191]. Notably, this analysis was limited by inter-study heterogeneity, potential confounding due to preferential carbapenem use in more acutely ill patients, and species-level variability in the risk of clinically significant AmpC production. Nonetheless, in view of cefepime’s favorable stability against relative AmpC hydrolysis, the high probability of PK/PD target attainment with appropriate dosing, and the absence of compelling evidence of inferiority in clinical outcomes studies, the panel suggests cefepime as a preferred treatment option for infections caused by organisms at moderate risk of clinically significant AmpC production (Table 1). Because cefepime is generally active against AmpC-E, cefepime–enmetazobactam is also anticipated to retain activity; however, its use is preferentially reserved for infections caused by ESBL-E or organisms co-producing AmpC and ESBL enzymes.
Although cefepime may be effective for the treatment of AmpC-E infections, it is suboptimal against infections caused by ESBL-E, which is a consideration if both enzymes are produced by Enterobacterales (Question 1.5). Data are incomplete on the frequency of ESBL production by Enterobacterales at moderate risk of clinically significant AmpC production in the United States. An evaluation of consecutive E. cloacae isolates from 66 United States hospitals from 2019-2020 indicated that 3% (6/211) contained a blaCTX-M gene [14]. A study from Pennsylvania found that 33% (15/45) of E. cloacae bloodstream isolates collected between 2003-2005 produced SHV-type ESBLs [193]. However, there was no association between ESBL production and the cefepime MIC. A study from Maryland found that ESBL genes were identified in 22% of K. aerogenes (4/18), 14% of E. cloacae (7/51), and in no C. freundii (0/8) bloodstream isolates collected between 2018-2021[194]. There was no correlation between the presence of an ESBL gene and the cefepime MIC; none of the ESBL-producing isolates had cefepime MICs of 4-8 µg/mL. Contemporary data specific to the United States are needed to better understand how frequently ESBLs are produced by Enterobacterales at moderate risk of clinically significant AmpC production. Available evidence does not suggest an association between cefepime susceptible dose-dependent MICs (i.e., MICs 4-8 µg/mL) and ESBL production. Accordingly, the panel suggests cefepime as a preferred treatment option for AmpC-E infections when the cefepime MIC is ≤8 µg/mL, provided an ESBL gene has not been identified.
Question 2.4: What is the role of ceftriaxone for the treatment of infections caused by Enterobacterales at moderate risk of clinically significant AmpC production due to an inducible ampC gene?
Suggested approach: Ceftriaxone (or cefotaxime or ceftazidime) is not suggested for the treatment of invasive infections caused by organisms at moderate risk of clinically significant AmpC production (i.e., E. cloacae complex, K. aerogenes, C. freundii, H. alvei). In cases of non-severe infection in which ceftriaxone was initiated empirically, and the patient demonstrates clinical improvement with adequate source control, continuation of ceftriaxone to complete the treatment course may be reasonable.
Rationale
Clinical reports vary in their estimates of how often resistance to ceftriaxone arises during treatment of infections caused by Enterobacterales considered to be at moderate risk for clinically significant AmpC induction. Interpreting the available evidence is complicated by several methodological and biological challenges. First, no CLSI-endorsed methods or FDA-cleared devices exist for the detection of ampC genes or AmpC enzymes in clinical isolates, precluding definitive confirmation of AmpC production. Second, ceftriaxone resistance may result from alternative mechanisms (e.g., ESBL production); yet this has been minimally investigated outside of E. coli, K. pneumoniae, and K. oxytoca. Third, many studies aggregate data from species at low risk for AmpC-mediated ceftriaxone resistance (e.g., S. marcescens) with those at higher risk (e.g., E. cloacae), thereby obscuring species-specific estimates of the likelihood of ceftriaxone resistance emergence. Fourth, studies assessing resistance following ceftriaxone exposure often omit molecular confirmation of relatedness between index and subsequent isolates. Moreover, several investigations employed pre-2010 CLSI ceftriaxone breakpoints (MIC ≤8 µg/mL), complicating the extrapolation of findings to current standards (MIC ≤1 µg/mL)[21]. Finally, substantial heterogeneity across studies, including variation in infection sources, illness severity, comorbidities, concomitant antibiotic therapy, and ceftriaxone dosing and duration, further limits the interpretability of clinical data.
These limitations notwithstanding, combining available data, the emergence of resistance after ceftriaxone exposure occurs in approximately 20% of infections caused by E. cloacae, K. aerogenes, or C. freundii [158, 166-168, 195]. Similar clinical data are lacking for H. alvei. An individual patient’s risk may differ based on host factors (e.g., higher with a persistent source of infection or prolonged durations of therapy).
No clinical trials have compared the outcomes of patients with presumed AmpC-E infections treated with ceftriaxone compared to alternate agents (e.g., cefepime). Several observational studies compared the clinical outcomes of patients with infections caused by E. cloacae, K. aerogenes, and C. freundii treated with ceftriaxone compared to either cefepime or carbapenems [172, 196-199]; two of the five cohorts demonstrated poorer clinical outcomes with the use of ceftriaxone [172, 199, 200]. Based on the available data, the panel suggests generally avoiding third-generation cephalosporins when treating infections caused by organisms at moderate risk of clinically significant AmpC production. However, for relatively uncomplicated infections it may be reasonable to transition to ceftriaxone after clear clinical improvement has been achieved and if there are no concerns for ongoing sources of infection (e.g., abscesses, indwelling catheters), weighing the convenience of once-daily ceftriaxone dosing with the potentially increased risk of emergence of resistance and possible treatment failure.
Question 2.5: What is the role of piperacillin-tazobactam for the treatment of infections caused by Enterobacterales at moderate risk of clinically significant AmpC production due to an inducible ampC gene?
Suggested approach: Piperacillin-tazobactam is not suggested for the treatment of invasive infections caused by Enterobacterales at moderate risk of clinically significant inducible AmpC production.
Rationale
Tazobactam is less effective at protecting β-lactams from AmpC hydrolysis than newer β-lactamase inhibitors, such as avibactam and relebactam [136]. As an example, in an in vitro study of E. cloacae isolates, tazobactam (paired with ceftolozane) was able to inhibit 100% (32/32) of wild-type, 67% (6/9) of ESBL, and only 19% (10/53) of AmpC-producing E. cloacae isolates [201]. In another study, increasing levels of ampC expression were associated with dramatic increases in piperacillin-tazobactam MICs[180]. Regarding clinical data, a 2019 meta-analysis summarized the findings of 12 observational studies, building upon a previous meta-analysis[190], and did not identify a difference in mortality between patients treated with piperacillin-tazobactam versus carbapenems for bacteremia caused by Enterobacter spp., Citrobacter spp., Serratia spp., Providencia spp., or Morganella spp. [202]. However, moderate heterogeneity across studies and confounding by indication likely existed (i.e., ill appearing patients were more likely to be prescribed carbapenems). At least three observational studies published after this meta-analysis, including 759 patients, suggest poorer outcomes for patients receiving piperacillin-tazobactam compared with cefepime and/or carbapenems [172, 203, 204].
A clinical trial compared the outcomes of 72 patients with bloodstream infections caused by Enterobacter spp., K. aerogenes, C. freundii, M. morganii, Providencia spp., or S. marcescens randomized to piperacillin-tazobactam or meropenem [205]. There were no significant differences in the primary outcome (a composite outcome including 30-day mortality, clinical failure, microbiological failure, or microbiological relapse) between study arms. However, some notable and seemingly conflicting findings were observed for individual components of this composite outcome: mortality (0% [0/38] versus 6% [2/34]); clinical failure (21% [8/38] versus 12% [4/34]); microbiological failure (13% [5/38] versus 0% [0/34]), and microbiological relapse (0% [0/38] versus 9% [3/34]) for the piperacillin-tazobactam and meropenem arms, respectively. The findings of this trial are challenging to interpret and a larger trial is needed to determine the role of piperacillin-tazobactam for the treatment of organisms at moderate risk for clinically significant ampC induction.
In light of the limited ability of tazobactam to protect piperacillin from AmpC hydrolysis in vitro and at least a few observational studies suggesting poorer clinical outcomes with the use of piperacillin-tazobactam compared to cefepime/carbapenems, the panel suggests caution with prescribing piperacillin-tazobactam for serious infections caused by AmpC-E.
Question 2.6: What is the role of β-lactam agents with activity against carbapenem-resistant organisms for the treatment of infections caused by Enterobacterales at moderate risk of clinically significant AmpC production?
Suggested approach: Although aztreonam-avibactam, ceftazidime–avibactam, imipenem–relebactam, meropenem–vaborbactam, and cefiderocol are expected to be active against AmpC-E, their use should generally be reserved for infections caused by carbapenem-resistant organisms. Ceftolozane–tazobactam is not suggested for the treatment of AmpC-E infections.
Rationale
Avibactam, vaborbactam, and relebactam have been shown to inhibit AmpC enzymes [137, 206-208]. Likewise, cefiderocol generally retains activity against AmpC-E [209]. Nonetheless, resistance to ceftazidime–avibactam among AmpC-E has been reported, most often driven by amino acid substitutions that expand the AmpC substrate-binding pocket, thereby improving accommodation of cephalosporins such as ceftazidime and cefiderocol [210-213]. The frequency with which AmpC-E acquire resistance to ceftazidime–avibactam remains undefined.
Carbapenems are typically stable to AmpC-mediated hydrolysis; consequently, imipenem-relebactam and meropenem-vaborbactam are expected to retain activity against AmpC-E. Although aztreonam-avibactam, ceftazidime-avibactam, imipenem-relebactam, meropenem-vaborbactam, and cefiderocol are likely to be effective therapeutic options, the panel advises reserving these agents for infections caused by carbapenem-resistant organisms, where they are most needed.
Ceftolozane was engineered to confer greater stability to hydrolysis by pseudomonal AmpC cephalosporinases (i.e., Pseudomonas-derived cephalosporinases) compared to earlier cephalosporins such as ceftazidime [214]. However, considerably less is known regarding ceftolozane-tazobactam’s activity against AmpC-E. Tazobactam provides relatively weak protection against AmpC-mediated hydrolysis compared with newer β-lactamase inhibitors, such as avibactam and relebactam (Question 2.5). Limited in vitro data suggest that ceftolozane-tazobactam may retain some activity against AmpC-E [215]; however, in at least one investigation, the agent was active against only 19% (10/53) of E. cloacae isolates producing moderate levels of AmpC enzymes [201]. Based on the available evidence, the panel does not suggest the use of ceftolozane-tazobactam for the treatment of AmpC-E infections. In the context of polymicrobial infections where both DTR P. aeruginosa and AmpC-E are isolated, ceftolozane-tazobactam may be considered as a therapeutic option to minimize exposure to multiple agents and their associated toxicities. If this approach is pursued, close clinical monitoring is suggested to ensure an appropriate response.
Question 2.7: What is the role of non-β-lactam agents for the treatment of infections caused by Enterobacterales at moderate risk of significant AmpC production due to an inducible ampC gene?
Suggested approach: Non-β-lactam agents are not substrates for AmpC enzymes and, therefore, remain effective treatment options against AmpC-E when bacterial isolates test susceptible, if appropriate based on the site of infection, severity of illness, and agent-specific toxicities.
Rationale
For AmpC-E uUTI, preferred treatment options include nitrofurantoin or TMP-SMX (Question 1.1). Alternative options include single-dose aminoglycosides, ciprofloxacin, levofloxacin, pivmecillinam, and sulopenem (Question 1.1). Mecillinam (the active moiety of pivmecillinam) and sulopenem demonstrate in vitro activity against >90% of AmpC-E isolates [39, 216-221]; however, clinical outcomes data are limited. In contrast, susceptibility data for gepotidacin against AmpC-E are comparatively sparse, and available evidence suggests elevated MICs among common AmpC-E isolates [29]. In the absence of confirmed susceptibility testing, gepotidacin is not suggested for the treatment of AmpC-E uUTI.
For cUTI, ciprofloxacin, levofloxacin, or TMP-SMX are preferred agents (Question 1.2), with aminoglycosides and sulopenem as alternative options (Question 1.2). Because TMP-SMX and fluoroquinolones are not substrates for AmpC-mediated hydrolysis, oral transition therapy with ciprofloxacin, levofloxacin, or TMP-SMX may be considered for invasive AmpC-E infections once susceptibility has been confirmed and clinical stability occurs (Question 1.3).
Section 3: Carbapenem-Resistant Enterobacterales (CRE)
CRE are members of the Enterobacterales order that are resistant to at least one carbapenem (i.e., ertapenem, imipenem, meropenem) or that produce a carbapenemase enzyme [222]. Certain Enterobacterales, including Morganella spp., Proteus spp., and Providencia spp., exhibit decreased susceptibility to imipenem due to structural characteristics of their penicillin-binding proteins (PBPs) that reduce the antibiotic’s binding affinity [223, 224]. Consequently, for these species, resistance to at least one carbapenem other than imipenem is required for classification as CRE.
CRE represent a heterogeneous group that can be broadly categorized as non-carbapenemase-producing or carbapenemase-producing. Non-carbapenemase-producing CRE typically arise from amplification of non-carbapenemase β-lactamase genes (e.g., blaCTX-M, ampC) in combination with outer membrane porin loss (e.g., OmpC/OmpF in E. coli or E. cloacae; OmpK35/OmpK36 in K. pneumoniae) [225, 226].
Carbapenemase-producing isolates account for 35%-83% of CRE cases in the United States, with higher proportions observed when CRE definitions require resistance to meropenem or imipenem [227-230]. The epidemiology of carbapenemase-producing Enterobacterales in the United States continues to evolve. Although blaKPC has historically most commonly been identified in K. pneumoniae isolates, blaKPC is increasingly detected in other species, including E. cloacae and E. coli [230]. Since 2021, a marked increase in New Delhi metallo-β-lactamase-producing Enterobacterales (NDM-E) has been observed, along with a more gradual increase in OXA-48-like producers (OXA-48-E) [229, 231]. KPC and OXA-48-like enzymes are serine carbapenemases, whereas NDM, Verona integron-encoded metallo-β-lactamases (VIM), and imipenem-hydrolyzing metallo-β-lactamases (IMP) are collectively classified as metallo-β-lactamase (MBL) carbapenemases. These enzyme classes differ fundamentally in catalytic mechanism: serine β-lactamases use an active-site serine to hydrolyze β-lactams, while MBLs depend on one or two zinc ions at the catalytic site, which coordinate and activate a water molecule for nucleophilic attack [232].
Carbapenemase families, and sometimes specific variants within a carbapenemase family, differ in β-lactam substrate profiles and susceptibility to inhibition by β-lactamase inhibitors. Consequently, identification of the specific carbapenemase family (e.g., KPC) produced by an organism causing infection optimizes therapeutic decision making to ultimately improve patient outcomes [233-236]. Treatment suggestions for CRE infections assume that in vitro activity of preferred or alternative agents has been demonstrated.
Question 3.1: What are preferred antibiotics for the treatment of uUTIs caused by CRE?
Suggested approach: Aminoglycosides (as a single dose), ciprofloxacin, levofloxacin, nitrofurantoin, or TMP-SMX are preferred treatment options for uUTIs caused by CRE, acknowledging the likelihood of CRE susceptibility to several of these agents may be low. Colistin, oral fosfomycin (for E. coli only), gepotidacin, or pivmecillinam are alternative options; there is also a low likelihood of CRE susceptibility to several of these agents. Several IV agents (e.g., aztreonam-avibactam, cefiderocol, ceftazidime-avibactam, fosfomycin [preferentially for E. coli], imipenem-relebactam, meropenem-vaborbactam) are likely to be effective, but it is suggested that their use be preserved for situations where resistance, availability, or intolerance preclude the use of other options.
Rationale
Because treatment courses for uUTI are relatively short and susceptibility data, particularly for newer oral uUTI agents, may not be available, therapy for CRE uUTI is frequently initiated and completed before carbapenem resistance is recognized. Review of prior urine culture results is therefore essential when evaluating patients with suspected uUTI to determine whether empiric CRE coverage is warranted [237]. Although several oral agents may retain activity against CRE, susceptibility rates are generally low, necessitating close clinical monitoring when these agents are used empirically. More comprehensive discussions of mechanisms of action, resistance patterns, and clinical efficacy are provided in Question 1.1.
Single-dose aminoglycosides are preferred agents given their renal elimination and high urinary concentrations, which support clinical efficacy in uUTI [26, 27]. United States surveillance data suggest CRE have variable susceptibility to aminoglycosides: amikacin (59%), gentamicin (47%), plazomicin (97%), and tobramycin (27%) [238]. Even in the setting of elevated MICs, urinary concentrations may theoretically exceed resistance thresholds and translate to clinical success [239].
Ciprofloxacin, levofloxacin, nitrofurantoin, and TMP-SMX are also preferred, based on favorable urinary pharmacokinetics, clinical trial data, and extensive clinical experience [37, 64-66]. However, available data suggest that fewer than 20% of CRE isolates are susceptible to fluoroquinolones or TMP-SMX, and approximately 30% to nitrofurantoin [238, 240-243].
Colistin is converted from its inactive prodrug, colistimethate sodium, to its active form within the urinary tract, thereby making colistin, but not polymyxin B which is primarily cleared through nonrenal routes[244], an alternative option for uUTI [245, 246]. Notably, CLSI does not define a susceptible breakpoint for colistin against Enterobacterales; MICs ≤2 µg/mL are categorized as intermediate [21]. Given the high urinary concentrations achieved, colistin is nevertheless anticipated to retain activity for infections confined to the urinary tract. In a United States collection of 117 CRE isolates, approximately 91% had colistin MICs within the intermediate range [238]. Despite this potential activity, colistin is suggested only as an alternative rather than a preferred option for CRE uUTI due to its toxicity profile. Even with relatively short treatment courses, the risk of nephrotoxicity is approximately 30% [247-250].
Oral fosfomycin is an alternative option for uUTI caused by carbapenem-resistant E. coli; it is not considered a preferred agent because clinical trial data demonstrate inferior outcomes compared with nitrofurantoin [37]. Susceptibility testing for fosfomycin is not routinely performed in many clinical microbiology laboratories, and contemporary United States data specifically evaluating activity against carbapenem-resistant E. coli are not available. Using the CLSI oral fosfomycin breakpoint (which differs from the IV breakpoint; Table 2), approximately 80% of carbapenem-resistant E. coli isolates are expected to be susceptible to oral fosfomycin [243, 251].
As discussed in Question 1.1, gepotidacin and pivmecillinam received approval for the treatment of uUTI in 2025. Data specifically evaluating gepotidacin activity against CRE isolates are extremely limited. However, given its novel mechanism of action targeting bacterial DNA gyrase and topoisomerase IV at sites distinct from fluoroquinolones, it is anticipated to retain activity against at least a subset of CRE isolates that are not susceptible to fluoroquinolones. In a surveillance study including approximately 600 AMR uropathogens, only a few of which were carbapenem-resistant, resistance to gepotidacin was observed in less than 1% of isolates [252]. Clinical outcomes data evaluating gepotidacin for uUTI caused by CRE are not available. Accordingly, gepotidacin is suggested as an alternative option.
Pivmecillinam is distinct from other oral agents suggested for CRE uUTI in that it is a β-lactam antibiotic, administered as the prodrug of the microbiologically active compound, mecillinam. In a collection of CRE isolates, mecillinam susceptibility was 0% among 174 KPC producers, 71% among 1,094 NDM-E, and 84% among 4,042 OXA-48-E; susceptibility among 2,349 non–carbapenemase-producing CRE isolates was 70% [253]. A separate collection of 105 molecularly characterized CRE isolates demonstrated limited activity (<50%) against NDM-E and OXA-48-E and no activity against KPC-producing Enterobacterales (KPC-E) [254]. A murine UTI model suggested promising in vivo activity against NDM-E [255]. Given the apparent ability of KPC enzymes to hydrolyze mecillinam, knowledge of the likely carbapenemase mechanism involved should inform consideration of pivmecillinam. Clinical outcomes data against CRE are lacking. It is suggested as an alternative agent for uUTI caused by CRE, if the likelihood of KPC-production is low.
Although several IV agents (e.g., aztreonam-avibactam, cefiderocol, ceftazidime-avibactam, fosfomycin [particularly for E. coli], imipenem-relebactam, meropenem-vaborbactam) have demonstrated in vitro activity and clinical efficacy against CRE that cause uUTI [69, 70, 138, 256-262], the panel suggests preferentially reserving their use for invasive CRE infections.
Question 3.2: What are preferred antibiotics for the treatment of pyelonephritis or cUTI caused by CRE?
Suggested approach: Ciprofloxacin, levofloxacin, and TMP-SMX, are preferred treatment options for cUTIs caused by CRE, acknowledging the likelihood of CRE susceptibility to these agents is low. Several IV agents (e.g., aztreonam-avibactam, cefiderocol, ceftazidime-avibactam, imipenem-relebactam, meropenem-vaborbactam) are also preferred options, particularly when clinical instability is present. IV fosfomycin (preferentially for E. coli) and once-daily aminoglycosides (i.e., amikacin, gentamicin, plazomicin, or tobramycin) are alternative agents for the treatment of cUTI caused by CRE.
Rationale
Ciprofloxacin, levofloxacin, or TMP-SMX are preferred treatment options for cUTI caused by CRE only after susceptibility is demonstrated, given the overall low likelihood of activity (Question 3.1). IV agents, including aztreonam-avibactam, cefiderocol, ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam, are also preferred options, particularly in the setting of clinical instability, supported by in vitro susceptibility data and clinical trial evidence demonstrating non-inferiority to alternative regimens for the treatment of UTIs [138, 256-262]. Notably, the proportion of CRE isolates included across trials is low. Selection among these agents should be guided primarily by the specific carbapenemase mechanism identified, in addition to AST results (Questions 3.4 to 3.6).
IV fosfomycin is an alternative agent for the treatment of cUTI (preferably those caused by E. coli) exhibiting carbapenem resistance (Question 1.2), only after susceptibility is confirmed, as only about 50% of isolates are likely to be susceptible when applying IV fosfomycin breakpoints (Table 2) [251, 263]. Once-daily aminoglycosides (i.e., amikacin, gentamicin, plazomicin, and tobramycin) are also alternative agents for the treatment of CRE cUTI (Question 1.2); agent specific differences exist in their likelihood of activity against CRE isolates (Question 3.1). Although expected to be effective as they achieve high renal parenchymal concentrations [72], duration-dependent nephrotoxicity should be carefully considered [73, 74]. Aminoglycosides can be useful for completing treatment courses, given their prolonged renal cortical concentrations and the logistical advantages of once-daily dosing [77, 79] (Table 1, Supplemental Material).
Question 3.3: What are the preferred antibiotics for the treatment of invasive infections caused by CRE that are not carbapenemase producing?
Suggested approach: For invasive infections due to Enterobacterales isolates that do not produce carbapenemases and demonstrate susceptibility to meropenem and imipenem (MIC ≤ 1 µg/mL) but are not susceptible to ertapenem (MIC ≥ 1 µg/mL), administration of extended-infusion meropenem or imipenem is suggested. In cases where isolates are not susceptible to ertapenem and retain susceptibility to either meropenem or imipenem, but not both, use of the active carbapenem via extended infusion may be considered, provided the patient is not critically ill and adequate source control has been achieved. For infections caused by non-carbapenemase-producing Enterobacterales that lack susceptibility to all carbapenems, preferred therapeutic options include aztreonam-avibactam, ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam. Cefiderocol, eravacycline, and tigecycline are alternative options. Notably, tetracycline derivatives exhibit rapid tissue distribution with low serum and urinary concentrations, limiting their utility in bacteremia and UTIs and potentially contributing to poorer outcomes in these settings [264, 265].
Rationale
For infections caused by non-carbapenemase-producing Enterobacterales isolates that are susceptible to imipenem and meropenem (MIC ≤1 µg/mL) but resistant to ertapenem (MIC ≥1 µg/mL), extended-infusion imipenem or meropenem is suggested. Surveillance data from a United States CRE isolate collection demonstrated that fewer than 3% of 1,249 isolates exhibiting ertapenem resistance while retaining susceptibility to meropenem and imipenem harbored a carbapenemase gene [266]. Instead, such isolates frequently exhibit amplification of non-carbapenemase β-lactamase genes (e.g., ESBLs or narrow-spectrum β-lactamases), typically in the presence of porin disruption, which have already attenuated ertapenem activity. Increasing β-lactamase production has the theoretical potential to compromise imipenem or meropenem efficacy over the course of therapy [225, 267]. Accordingly, when extended-infusion carbapenem therapy is employed in this setting, close clinical monitoring is warranted. For uUTI caused by isolates with this phenotype, standard-infusion imipenem or meropenem may be a reasonable alternative.
In situations where isolates are non-carbapenemase-producing and susceptible to one carbapenem but not another (e.g., susceptible to imipenem but resistant to meropenem, or vice versa), evidence to guide optimal management is limited. In such cases, treatment decisions should be individualized based on patient-specific factors. In critically ill patients or in the presence of ongoing infection sources, consideration may be given to newer β-lactam/β-lactamase inhibitor combinations, as the inhibitor component may mitigate carbapenem hydrolysis secondary to significant β-lactamase (e.g., ESBL, CMY, OXA-1) expression[268].
For isolates that are non-carbapenemase-producing yet not susceptible to any carbapenem, newer β-lactam agents are preferred, including aztreonam-avibactam, ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam, with agent selection guided by AST results. Among these, there is modest panel preference for ceftazidime-avibactam and imipenem-relebactam, as in vitro data suggest that avibactam and relebactam may demonstrate somewhat greater inhibitory activity in this context compared with vaborbactam [269, 270]. Cefiderocol may also demonstrate activity against such isolates; however, its lack of a companion β-lactamase inhibitor raises theoretical concerns of its effectiveness in the setting of high-level β-lactamase expression. Consequently, cefiderocol is considered an alternative option in these scenarios.
Eravacycline and tigecycline may serve as alternative options for CRE infections that do not involve the bloodstream or urinary tract (Question 3.7). Their antibiotic activity is independent of carbapenemase production status.
Question 3.4: What are the preferred antibiotics for the treatment of invasive infections caused by KPC-producing Enterobacterales?
Suggested approach: Ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam are preferred treatment options for KPC-E infections. Among these, resistance emergence during therapy has been reported in approximately 10% of cases with ceftazidime-avibactam, compared with <3% for imipenem-relebactam and meropenem-vaborbactam. Aztreonam-avibactam, cefiderocol, eravacycline, and tigecycline are alternative options, with eravacycline and tigecycline not suggested for infections involving the bloodstream or urinary tract.
Rationale
Preferred agents for KPC-E infections include ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam. Although no clinical trials directly comparing these agents are available, they have consistently been associated with improved clinical outcomes and significantly less toxicity compared with alternative regimens, which were commonly polymyxin- or aminoglycoside-based [233, 271-275].
United States surveillance data indicate that ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam demonstrate greater than 95% activity against KPC-E [276]. While all three are preferred options, the panel slightly favors meropenem-vaborbactam, followed by ceftazidime-avibactam, and then imipenem-relebactam. This ranking reflects composite observational data suggesting numerically more favorable clinical outcomes with meropenem-vaborbactam compared with ceftazidime-avibactam, along with a lower likelihood of resistance emergence, although these differences were generally not statistically significant [277-279].
In one observational study of patients with CRE infections (approximately 73% KPC-E), 30-day survival was 81% (85/105) in the ceftazidime-avibactam group and 88% (23/26) in the meropenem-vaborbactam group; clinical cure occurred in 62% (65/105) and 69% (18/26), respectively [279]. Among patients with recurrent infections, resistance emerged in 20% (3/15) of those receiving ceftazidime-avibactam and in none (0/3) receiving meropenem-vaborbactam. In a second observational study, 30-day survival was 73% (38/52) with ceftazidime-avibactam versus 81% (29/36) with meropenem-vaborbactam; patients receiving meropenem-vaborbactam had approximately twice the odds of a favorable clinical response at 72 hours [277]. Estimates of resistance emergence were not reported. In a third observational study of 73 patients with invasive KPC-E infections, overall survival did not differ between groups; however, among patients with recurrent infection within 90 days, resistance developed in 12% (2/17) of those treated with ceftazidime-avibactam and in none (0/7) treated with meropenem-vaborbactam [278]. Clinical cure was not reported.
Comparative clinical data evaluating imipenem-relebactam against either ceftazidime-avibactam or meropenem-vaborbactam for KPC-E infections are lacking. In an uncontrolled observational study including six patients with invasive KPC-E infections, all patients survived and achieved clinical cure with imipenem-relebactam [280]. However, in a clinical trial of imipenem-non-susceptible Enterobacterales infections, favorable clinical response occurred in only 40% (2/5) of patients treated with imipenem-relebactam [274]. Although the sample size precludes definitive conclusions, these trial results warrant caution. Nevertheless, the demonstrated in vitro activity of imipenem-relebactam against KPC-E isolates, extensive clinical experience with imipenem, and the inhibitory potential of relebactam [281] collectively support the expectation of clinical efficacy of imipenem-relebactam for KPC-E infections.
A shared vulnerability of ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam is amplification of blaKPC, which increases enzyme expression and hydrolytic capacity, thereby diminishing β-lactam activity [282]. Resistance emergence during ceftazidime-avibactam therapy has been reported in approximately 10% of cases [282-286]. The predominant mechanism involves substitutions within or adjacent to the KPC Ω-loop, and less commonly alterations in AmpC enzymes [282]. These changes remodel the active site, enhancing ceftazidime hydrolysis while reducing avibactam binding. Notably, ceftazidime-avibactam-resistant KPC variants frequently exhibit collateral reductions in carbapenem MICs, occasionally restoring in vitro carbapenem susceptibility [287-291]; the clinical significance of this phenotypic reversion remains unclear. In contrast, resistance during imipenem-relebactam or meropenem-vaborbactam therapy is reported in <3% of cases and is primarily mediated by reduced outer membrane permeability (e.g., disruptions of the ompK35 and ompK36 porin genes in K. pneumoniae) [282, 292-298].
Aztreonam-avibactam and cefiderocol are alternative agents for KPC-E infections. Both demonstrate greater than 95% in vitro activity against KPC-E isolates [299-301]. Clinical data supporting aztreonam-avibactam for KPC-E infections are very limited [302]. In a subgroup analysis of a clinical trial comparing cefiderocol with alternative regimens (primarily polymyxin-based therapy), survival in the KPC-E subgroup was 78% (7/9) with cefiderocol versus 79% (11/14) with alternative therapy [259].
Eravacycline and tigecycline are additional alternative options for KPC-E infections that do not involve the bloodstream or urinary tract, although clinical data are limited (Question 3.7). Their activity is independent of the presence or type of carbapenemase.
Question 3.5: What are the preferred antibiotics for the treatment of invasive infections caused by NDM-producing Enterobacterales?
Suggested approach: Aztreonam-avibactam and cefiderocol are preferred treatment options for NDM-E infections. If aztreonam-avibactam is not available, ceftazidime-avibactam plus aztreonam is an alternative. Eravacycline and tigecycline are alternative options for infections not involving the bloodstream or urinary tract.
Rationale
Aztreonam-avibactam and cefiderocol are the preferred agents for infections caused by NDM-E. NDM enzymes belong to the larger category of MBL enzymes and hydrolyze all traditional β-lactam antibiotics except aztreonam [303]. Despite its stability to hydrolysis by NDM, aztreonam remains susceptible to hydrolysis by serine β-lactamases frequently co-produced by NDM-E isolates (e.g., ESBLs, AmpCs, OXA-type enzymes)[303]. Avibactam inhibits these serine β-lactamases, thereby protecting aztreonam from enzymatic degradation and permitting it to reach its primary target, PBP3. Notably, the preferred agents for KPC-E are ineffective against NDM-E because neither avibactam, relebactam, nor vaborbactam inhibit NDM.
Using the CLSI susceptibility breakpoint of ≤4/4 µg/mL (Table 2), surveillance data indicate that more than 95% of NDM-E isolates are susceptible to aztreonam-avibactam [228, 304-306]. The suggested loading and subsequent maintenance dosing of aztreonam-avibactam is supported by population PK/PD modeling incorporating joint pharmacodynamic targets (≥60% fT>MIC for aztreonam and ≥50% fT>2.5 µg/mL for avibactam), as well as animal model data [307-309] (Table 1).
Clinical outcome data for aztreonam-avibactam remain limited and derive primarily from subgroup analyses of two trials [302, 310]. In one subgroup analysis of six patients with NDM-E infections, clinical cure occurred in 33% (2/6) of patients treated with aztreonam-avibactam compared with 0% (0/1) in the meropenem arm; 28-day survival was 83% (5/6) and 100% (1/1), respectively [302]. In a second clinical trial that included 11 patients with NDM-E infections, clinical cure was observed in 44% (4/9) of patients receiving aztreonam-avibactam versus 0% (0/2) receiving alternative therapy (polymyxin- or aminoglycoside-based regimens); 28-day survival was 89% (8/9) and 50% (1/2), respectively [310].
When aztreonam-avibactam is not available, ceftazidime-avibactam plus aztreonam is a reasonable alternative [303]. Although no direct clinical comparisons exist, available data do not clearly favor one regimen over the other. It has been hypothesized that any residual ceftazidime activity - via affinity for additional PBPs (PBP1a, PBP1b, PBP2) - beyond ceftazidime’s primary affinity for PBP3 - may enhance bactericidal effects beyond aztreonam alone, though this remains unproven[311]. In a study of 102 adults with MBL-producing bloodstream infections (82 NDM-producing), 30-day survival was 81% (42/52) with ceftazidime-avibactam plus aztreonam versus 56% (28/50) with polymyxin- or tigecycline-based therapy[312]. In another cohort including 328 NDM-E isolates, 30-day survival was 78% (167/215) with ceftazidime-avibactam, compared with 67% (22/33) for cefiderocol and 50% (13/26) for colistin[313]. A validated MIC testing method for ceftazidime-avibactam plus aztreonam is not available; however, the CLSI-endorsed broth disk elution method can be used to determine susceptibility [21, 314]. Strategies for administering ceftazidime-avibactam plus aztreonam [315-317] are summarized in Table 1 and the Supplemental Material.
In a study of healthy volunteers given ceftazidime-avibactam ± aztreonam, asymptomatic transaminase elevations occurred in 40% of participants and resolved with drug cessation [317]. Elevations were dependent on aztreonam dosing, occurring primarily in groups receiving aztreonam 8 grams per day either as a continuous infusion or every 6 hours; transaminitis was not increased with the co-administration of ceftazidime-avibactam. Asymptomatic transaminase elevations occurred in approximately 6% of patients in aztreonam-avibactam trials where the total daily dose of aztreonam was 6 grams per day [302, 310].
Despite comparable in vitro activity between ceftazidime-avibactam plus aztreonam and aztreonam-avibactam, the fixed 3:1 aztreonam-avibactam formulation ensures synchronized β-lactam/β-lactamase inhibitor exposure and improves probability of joint target attainment [309]. In addition, single-agent administration enhances feasibility. For these reasons, the panel preferentially suggests aztreonam-avibactam when available. Notably, although in vitro data suggest that combining aztreonam with meropenem-vaborbactam or imipenem-relebactam may provide activity against NDM-E [318, 319], clinical experience with these combinations remains limited [320].
Cefiderocol is a catechol-substituted siderophore cephalosporin that co-opts bacterial iron acquisition pathways to facilitate periplasmic entry via active ferric iron transport systems [321]. Once internalized, cefiderocol demonstrates high-affinity binding predominantly to PBP3, thereby inhibiting peptidoglycan cross-linking, impairing cell wall biosynthesis, and ultimately inducing bacterial cell lysis. United States surveillance data indicate that cefiderocol retains activity against approximately 85% of NDM-E isolates [322, 323].
Clinical data evaluating cefiderocol in infections due to NDM-E are limited. A subgroup of patients enrolled in two clinical trials with NDM-E infections demonstrated higher proportions of clinical cure with cefiderocol compared with alternative therapy (primarily polymyxin-based regimens), 60% (6/10) versus 20% (1/5), respectively, as well as improved 28-day survival, 90% (9/10) versus 40% (2/5)[324]. Conversely, in a separate trial evaluating a subgroup of patients with NDM-E bloodstream infections, 30-day survival was 50% (8/16) in the cefiderocol arm compared with 82% (9/11) in the alternative therapy arm, again largely polymyxin-based [325].
Direct comparative data evaluating aztreonam-avibactam versus cefiderocol for the treatment of infections caused by NDM-E are not available. Both agents are mechanistically rational options in this setting; however, clinical data supporting their use are limited and derived primarily from small subgroup analyses, with variable and, in some cases, suboptimal outcomes. In the absence of evidence demonstrating superiority of one regimen over the other, both aztreonam-avibactam and cefiderocol are considered preferred therapeutic options.
For both aztreonam-avibactam and cefiderocol, resistance in NDM-producing E. coli isolates is strongly associated with specific four-amino acid insertions in PBP3 (e.g., YRIN, YRIK), particularly when combined with CMY-type AmpC variants [326-330]. These insertions reduce affinity for aztreonam, ceftazidime, and cefiderocol, compromising the activity of these agents. Although first recognized as a major concern in Asia, these mutants are emerging in the United States and have been described in approximately 30% of NDM-producing E. coli isolates in the mid-Atlantic region [331]. When NDM-producing E. coli with resistance to both aztreonam-avibactam and cefiderocol are encountered, clinical data to inform optimal therapeutic management remain limited; in such circumstances, individualized combination regimens incorporating agents such as IV fosfomycin, polymyxin B, and/or tigecycline warrant consideration.
In NDM-producing K. pneumoniae, resistance to aztreonam-avibactam is less common than in E. coli, but reported mechanisms include permeability changes (e.g., porin loss, increased efflux) and mutations in plasmid-encoded AmpC β-lactamases, particularly CMY variants [332, 333]. As aztreonam-avibactam has only recently entered clinical use, further data on resistance mechanisms and frequency are anticipated.
Beyond PBP3 insertions with CMY variants, cefiderocol resistance has been associated with mutations in the TonB-dependent iron transport system [334-337] and increased expression of NDM enzymes [338, 339]. Data suggest that rates of cefiderocol resistance development may vary by MBL family and even by specific NDM allele [232].
Eravacycline and tigecycline represent alternative therapeutic options for NDM-E infections that do not involve the bloodstream or urinary tract, although clinical data are limited (Question 3.7).
Question 3.6: What are the preferred antibiotics for the treatment of invasive infections caused by CRE if OXA-48-like production is present?
Suggested approach: Ceftazidime-avibactam is the preferred treatment option for OXA-48-E infections. Aztreonam-avibactam, cefiderocol, eravacycline, and tigecycline are alternative treatment options, with eravacycline and tigecycline not suggested for infections involving the bloodstream or urinary tract.
Rationale
Ceftazidime-avibactam is the preferred treatment for infections caused by OXA-48-E. In vitro data demonstrate that over 95% of OXA-48-E isolates are susceptible to ceftazidime-avibactam [340, 341]. Clinical outcomes data are limited to observational studies.
In a single-arm observational cohort of 171 patients with OXA-48-E infections treated with ceftazidime-avibactam, 79% (135/171) achieved clinical cure, and 78% (134/171) were alive at day 30 [342]. In a second observational study of 76 patients with OXA-48-E bloodstream infections, clinical success was observed in 91% (30/33) of patients treated with ceftazidime-avibactam compared with 58% (25/43) of those receiving alternative regimens (predominantly polymyxin-based therapies). Thirty-day survival was 88% (29/33) in the ceftazidime-avibactam group and 74% (32/43) in the comparator group[343]. Unlike avibactam, both vaborbactam and relebactam demonstrate limited inhibitory activity against OXA-48-like enzymes [344-347]. In a neutropenic thigh infection model evaluating 51 OXA-48-E isolates, the in vivo activity of ceftazidime-avibactam was consistently greater than that of meropenem-vaborbactam or imipenem-relebactam, regardless of MIC values [345]. Accordingly, meropenem-vaborbactam and imipenem-relebactam are not suggested treatment options for OXA-48-E isolates, even when in vitro susceptibility is reported.
Published clinical reports describing treatment-emergent resistance during ceftazidime-avibactam therapy for OXA-48-E infections remain exceedingly sparse. However, in vitro-selected resistant mutants suggest that resistance may arise through alterations in efflux pump systems, modifications or loss of outer membrane porins, structural changes in PBP3, and/or amino acid substitutions within OXA-48-like β-lactamases; the clinical significance of these observations is unknown [348, 349].
Aztreonam-avibactam and cefiderocol represent alternative therapeutic options for OXA-48-E infections. Both agents are active against over 95% of OXA-48-E isolates [45, 299, 301]. Clinical outcomes data for aztreonam-avibactam in OXA-48-E infections are lacking and clinical data for cefiderocol are limited. In a subgroup analysis of 10 patients with OXA-48-E infections enrolled in two clinical trials and treated with cefiderocol, 70% (7/10) achieved clinical cure, and 100% (10/10) were alive at day 28[350].
Eravacycline and tigecycline are also considered alternative options for OXA-48-E infections that do not involve the bloodstream or urinary tract (Question 3.7).
Question 3.7: What is the role of tetracycline derivatives for the treatment of infections caused by CRE?
Suggested approach: Although β-lactam agents remain preferred treatment options for invasive CRE infections, eravacycline and tigecycline are alternative options when β-lactam agents are either not active or unable to be tolerated. Tetracycline derivatives are not suggested for the treatment of CRE urinary tract or bloodstream infections.
Rationale
Tetracycline derivatives retain activity against CRE isolates independent of carbapenemase production [240]. Resistance is commonly mediated by efflux pump overexpression (e.g., AcrAB-TolC) [351]. Tetracycline derivatives exhibit rapid tissue distribution with low serum and urinary concentrations, limiting their utility in bacteremia and UTIs and potentially contributing to poorer outcomes in these settings [264, 265]. Eravacycline and tigecycline may be considered for CRE infections in which tissue penetration is advantageous, such as intra-abdominal infections, skin and soft tissue infections, osteomyelitis, and pneumonia.
Tigecycline has substantially more clinical data for treating CRE infections than eravacycline [352-354]. Although direct comparisons with newer β-lactams are limited, observational data generally favor the newer β-lactams, although tigecycline was not consistently the comparator in these analyses [355]. Pharmacodynamic modeling and clinical data suggest that tigecycline MICs ≥0.5 µg/mL are associated with poor outcomes in CRE infections, despite remaining within the FDA susceptible range (≤2 µg/mL) [265, 356, 357] (Table 2). Thus, isolates reported as susceptible may still be associated with suboptimal clinical response. CLSI breakpoints are not established for tigecycline or eravacycline.
Clinical trial data evaluating eravacycline for CRE infections are limited, with fewer than five CRE cases included across studies [358, 359], and post-marketing data remain sparse [360]. Gastrointestinal intolerance is more frequent with tigecycline than with eravacycline; nausea occurs in approximately 20–25% of patients receiving tigecycline compared with about 5% with eravacycline [361].
Clinical data evaluating minocycline for CRE infections are also limited, and susceptibility proportions appear lower than for tigecycline or eravacycline [240, 362-364]. Although omadacycline demonstrates greater in vitro activity than minocycline [351, 365, 366], clinical outcome data for CRE infections are lacking. The panel suggests caution when considering minocycline or omadacycline for the treatment of CRE infections.
Question 3.8: What is the role of combination antibiotic therapy for the treatment of infections caused by CRE?
Suggested approach: Combination antibiotic therapy (i.e., the use of a β-lactam agent in combination with an aminoglycoside, fluoroquinolone, IV fosfomycin, tetracycline, or polymyxin) is not routinely suggested for the treatment of infections caused by CRE.
Rationale
While empiric combination therapy may increase the likelihood that at least one active agent is administered in patients at risk for CRE infection, available evidence does not support the continuation of combination therapy once a β-lactam agent with confirmed in vitro activity has been identified. Continued use of a second agent has not been shown to improve clinical outcomes and instead increases the risk of antibiotic-associated adverse events [367]. Furthermore, clinical data demonstrating that combination therapy prevents the emergence of resistance are lacking.
No clinical trials have compared novel β-lactam agents as monotherapy versus as components of combination regimens (e.g., ceftazidime-avibactam alone versus ceftazidime-avibactam plus tobramycin). The limited available observational data have not demonstrated improved outcomes with combination therapy [342, 368, 369]. The largest observational study evaluated 577 patients with KPC-E infections treated with either ceftazidime-avibactam monotherapy or ceftazidime-avibactam in combination with a second agent [369]. Thirty-day survival was comparable between groups - approximately 74% (122/165) in the monotherapy arm and 75% (309/412) in the combination arm - indicating no apparent survival advantage with combination therapy.
IV fosfomycin has been used for several decades in many regions, and observational data evaluating its use as part of combination therapy for CRE infections have yielded variable results [370-373]. Substantial heterogeneity across studies precludes definitive conclusions regarding its role. Although routine use of IV fosfomycin in combination regimens is not suggested, it may be considered in select cases of carbapenem-resistant E. coli infection when no active β-lactam agents are available (e.g., NDM-E with PBP3 insertions and CMY enzyme production resistant to both aztreonam-avibactam and cefiderocol). In such circumstances, IV fosfomycin is suggested only in combination with another active agent (e.g., tigecycline, polymyxin B), recognizing that supporting clinical data are limited.
Section 4: Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR P. aeruginosa)
Multidrug-resistant (MDR) P. aeruginosa is defined as P. aeruginosa that is not susceptible to at least one antibiotic in at least three antibiotic classes for which susceptibility is generally expected, including penicillins, cephalosporins, carbapenems, fluoroquinolones, and aminoglycosides [374]. Difficult-to-treat resistance (DTR) is defined as isolates exhibiting non-susceptibility to all the following agents: aztreonam, cefepime, ceftazidime, ciprofloxacin, imipenem, levofloxacin, meropenem, and piperacillin-tazobactam [375].
MDR and DTR P. aeruginosa generally arise through the interplay of multiple resistance mechanisms. These include decreased expression of outer membrane porins (e.g., OprD), increased production of, or amino acid substitutions within, Pseudomonas-derived cephalosporinase (PDC) enzymes (commonly referred to as pseudomonal AmpC enzymes), upregulation of efflux pumps (e.g., MexAB-OprM), mutations in PBP targets, the presence of ESBLs (e.g., blaOXA-10), and occasionally, although rarely in the United States, carbapenemase enzymes (e.g., VIM) [376].
Currently four β-lactam agents with potential activity against DTR P. aeruginosa are available in the United States. These include cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam. The panel encourages clinical microbiology laboratories to perform AST for all four agents when DTR P. aeruginosa isolates are identified in clinical cultures given the variable activity of the four agents against DTR P. aeruginosa. Treatment suggestions for DTR P. aeruginosa infections assume that in vitro activity of preferred or alternative agents has been demonstrated.
Question 4.1: What are preferred antibiotics for the treatment of infections caused by MDR P. aeruginosa?
Suggested approach: When P. aeruginosa isolates test susceptible to both traditional non-carbapenem β-lactam agents (i.e., aztreonam, cefepime, ceftazidime, piperacillin-tazobactam) and to carbapenems, the former are preferred over carbapenem therapy. For infections caused by P. aeruginosa isolates not susceptible to any carbapenem but susceptible to traditional β-lactams, the administration of a traditional non-carbapenem β-lactam is also suggested, using high dosages and prolonged infusions. For critically ill patients or those with poor source control with P. aeruginosa isolates resistant to carbapenems but susceptible to traditional β-lactams, use of newer β-lactam agents to which P. aeruginosa test susceptible (e.g., cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, imipenem-relebactam) is also a reasonable treatment approach.
Rationale
In general, when a P. aeruginosa isolate demonstrates in vitro susceptibility to traditional antipseudomonal β-lactam agents (e.g., aztreonam, cefepime, ceftazidime, piperacillin–tazobactam) or fluoroquinolones (e.g., ciprofloxacin, levofloxacin), the panel favors selection of an agent from these classes rather than carbapenem therapy, with the goal of preserving carbapenem activity for future infections caused by increasingly drug-resistant organisms. Notably, carbapenem use for P. aeruginosa infections has been associated with a higher likelihood of resistance emergence during therapy compared with other traditional antipseudomonal β-lactams [377, 378], without corresponding improvements in clinical outcomes [377].
MIC distributions for traditional β-lactam agents are generally higher for P. aeruginosa than for Enterobacterales [323]. For instance, the MIC distribution of wild-type P. aeruginosa isolates extends to 8 µg/mL for both cefepime and ceftazidime and to 16/4 µg/mL for piperacillin–tazobactam [379]. In contrast, wild-type E. coli isolates exhibit substantially lower MIC values, extending to 0.125 µg/mL, 1 µg/mL, and 8/4 µg/mL for cefepime, ceftazidime, and piperacillin–tazobactam, respectively [379].
Given relatively elevated β-lactam MICs, even among wild-type P. aeruginosa isolates, prolonged infusions may be required to maximize the proportion of the dosing interval during which free drug concentrations exceed the MIC, a key determinant of β-lactam efficacy and clinical success [380-383]. Consistent with these PK/PD principles, clinical data suggest improved patient outcomes with prolonged β-lactam infusions (e.g., 3-4 hours) compared with standard infusions (e.g., 30 minutes) for the treatment of P. aeruginosa infections [384, 385].
P. aeruginosa isolates that are not susceptible to carbapenems (e.g., imipenem or meropenem MICs ≥4 µg/mL) yet susceptible to other traditional antipseudomonal β-lactam agents account for at least 40% of carbapenem-resistant P. aeruginosa isolates [386, 387]. This resistance phenotype is most commonly attributable to reduced expression or alterations of the OprD porin, which mediates carbapenem entry across the outer membrane of P. aeruginosa into the periplasmic space [388, 389].
To date, comparative effectiveness data to inform optimal treatment strategies for infections caused by carbapenem-resistant P. aeruginosa isolates that retain susceptibility to traditional β-lactams (e.g., cefepime) are limited[390-392] and the optimal approach is unclear. In such cases, the panel’s preferred strategy is administration of a traditional β-lactam to which the organism is susceptible using a high-dose, extended-infusion regimen (e.g., cefepime 2 g IV every 8 hours infused over ≥3 hours) to optimize drug exposure (Table 1).
An alternative therapeutic strategy is the use of newer β-lactam agents (e.g., cefiderocol, ceftazidime-avibactam, ceftolozane–tazobactam, imipenem-relebactam). While the panel favors preserving their activity for future AMR infections, it is reasonable to consider their use for critically ill patients or in those with ongoing, uncontrolled sources of infection (e.g., large intra-abdominal abscess).
Regardless of the antibiotic selected, patients with P. aeruginosa infections should be closely monitored for clinical response, given this organism’s remarkable capacity to develop resistance through mutational and adaptive changes in gene expression during antibiotic exposure. In an evaluation of 767 episodes of P. aeruginosa bacteremia, emergence of resistance within 30 days occurred at the following frequencies for each agent: ceftazidime (12%), imipenem (27%), meropenem (15%), and piperacillin–tazobactam (8%) [378]. Accordingly, clinicians are encouraged to obtain repeat AST for subsequent P. aeruginosa isolates recovered from the same patient to guide ongoing therapeutic decision-making.
Question 4.2: What are preferred antibiotics for the treatment of cUTI caused by DTR P. aeruginosa?
Suggested approach: Cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam (listed alphabetically, no order of preference) are the preferred treatment options for cUTI caused by DTR P. aeruginosa. Once-daily amikacin or tobramycin are alternative agents for the treatment of DTR P. aeruginosa cUTI.
Rationale
Cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam are preferred therapies for cUTI caused by DTR P. aeruginosa, supported by clinical trials demonstrating non-inferiority compared with standard comparator regimens [138, 258, 259, 262, 393]. Available data are insufficient to preferentially suggest one agent over another. However, given cefiderocol’s unique activity compared to the other newer anti-pseudomonal β-lactams against NDM-E and non-fermenting gram-negative organisms beyond P. aeruginosa, consideration should be given to reserve its use for these other AMR infections. Treatment considerations for cUTI caused by P. aeruginosa isolates producing a carbapenemase are addressed in Question 4.4.
Once-daily amikacin or tobramycin are alternative agents for the treatment of DTR P. aeruginosa cUTI [245]. Although expected to be effective as they achieve high renal parenchymal concentrations [72], duration-dependent nephrotoxicity should be carefully considered [73, 74]. These agents are useful for completing treatment courses, given their prolonged renal cortical concentrations and the logistical advantages of once-daily dosing [77, 79] (Table 1, Supplemental Material). Notably, plazomicin’s in vitro activity against P. aeruginosa is comparable to or slightly inferior to amikacin; it does not offer improved activity over traditional aminoglycosides against this species [394]. Neither CLSI nor FDA breakpoints for plazomicin against P. aeruginosa are available (Table 2).
uUTI due to DTR P. aeruginosa is exceedingly uncommon. If identified, potential treatment options include a single dose of amikacin or tobramycin (Question 1.1), cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, imipenem-relebactam, or colistin, with the same caveats regarding cefiderocol as described for cUTI. Importantly, colistin, but not polymyxin B, is converted from its inactive prodrug, colistimethate sodium, to its active form within the urinary tract, thereby making colistin, but not polymyxin B, a potential therapeutic option for uUTI [245, 395].
Question 4.3: What are preferred antibiotics for the treatment of infections outside of the urinary tract caused by DTR P. aeruginosa?
Suggested approach: Ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam are the preferred agents for the treatment of infections outside of the urinary tract caused by DTR P. aeruginosa. Among these, ceftolozane-tazobactam is the preferred option for pneumonia caused by DTR P. aeruginosa. Cefiderocol is an alternative option for infections outside of the urinary tract caused by DTR P. aeruginosa.
Rationale
Ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam are preferred therapies for DTR P. aeruginosa, whereas cefiderocol is suggested as an alternative option. Clinical trials directly comparing these agents are not available. However, clinical trials have identified ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam to be associated with favorable clinical outcomes for pneumonia, where P. aeruginosa is a common pathogen [142, 152, 396]. Although these trials enrolled few patients with DTR P. aeruginosa, observational studies have consistently demonstrated improved patient outcomes with these newer agents for infections due to MDR or DTR P. aeruginosa compared with alternative regimens, which typically consist of combinations of polymyxins, aminoglycosides, and/or carbapenems [397-401].
In contrast, cefiderocol has not been found to be superior to alternative agents for infections due to AMR P. aeruginosa [259]. In a subgroup analysis of a randomized clinical trial that included 22 patients with carbapenem-resistant P. aeruginosa infections, survival was 82% in both the cefiderocol and alternative (primarily polymyxin-based) therapy arms [259]. Similarly, in another randomized trial comparing cefiderocol with traditional therapy, a subgroup of 16 patients with carbapenem-resistant P. aeruginosa bacteremia experienced identical 30-day survival of 75% in each treatment arm, with the alternative arm consisting of mostly polymyxin-based combinations [325]. Observational data assessing cefiderocol for the treatment of DTR P. aeruginosa infections are emerging; however, these studies are generally limited by small sample sizes and the absence of comparator groups, restricting their ability to inform relative effectiveness [402-404]. Accordingly, the panel suggests cefiderocol as an alternative option when inactivity or intolerance precludes the use of preferred β-lactam agents for infections outside of the urinary tract caused by DTR P. aeruginosa.
Several observational studies have compared outcomes among patients treated with ceftazidime-avibactam versus ceftolozane-tazobactam for DTR P. aeruginosa infections [405-408]. None of these studies identified differences in 30-day survival. However, some differences in clinical outcomes have been observed. The largest study which included patients with MDR P. aeruginosa pneumonia or bacteremia reported lower clinical success among the patients with pneumonia treated with ceftazidime-avibactam (51% [89/175]) versus ceftolozane-tazobactam (63% [110/175]) [407]. Across the overall cohort, ceftazidime-avibactam was also associated with a higher 30-day risk of recurrent infection (21% [44/210] versus 15% [31/210]). Another observational study reported higher rates of recurrent pneumonia with ceftazidime-avibactam 18% [21/117] versus ceftolozane–tazobactam (8% [6/80] [408]). Although these studies were observational and “clinical success” is a more subjective endpoint than mortality, particularly when it comes to non-fermenting gram-negatives and pneumonia, PK/PD differences between ceftazidime-avibactam and ceftolozane-tazobactam may explain these findings. Ceftolozane achieves epithelial lining fluid concentrations that are 50% of plasma concentrations and exceed 4 μg/mL (i.e., the ceftolozane susceptibility breakpoint) for 100% of the dosing interval in patients with pneumonia [409]. In contrast, both ceftazidime and avibactam achieve epithelial lining fluid concentrations of approximately 30% of plasma levels, which may be suboptimal given that ceftazidime-avibactam relies on adequate exposure of both components to achieve activity against DTR P. aeruginosa [410].
DTR P. aeruginosa isolates may be less likely to test susceptible to imipenem-relebactam compared to ceftolozane-tazobactam and ceftazidime-avibactam [411, 412]. Moreover, less clinical outcomes data are available for imipenem-relebactam. In an observational study of 63 patients with MDR P. aeruginosa infections, 30-day survival was approximately 80% [413]. Although no comparator arm was included, survival is similar to that observed with ceftazidime-avibactam and ceftolozane-tazobactam in cohort studies [405-408]. Based on available clinical outcomes data, ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam are all considered preferred agents for the treatment of DTR P. aeruginosa infections. However, the panelists prefer ceftolozane-tazobactam when treating DTR P. aeruginosa pneumonia.
Question 4.4: How does identification of carbapenemases produced by DTR P. aeruginosa influence treatment selection?
Suggested approach: Although carbapenemase production is currently uncommon among P. aeruginosa clinical isolates in the United States, carbapenemase identification has important therapeutic implications. For infections caused by KPC-producing P. aeruginosa, cefiderocol, ceftazidime-avibactam, and imipenem-relebactam, are preferred treatment options. Cefiderocol is the preferred agent for infections caused by P. aeruginosa producing NDM, VIM, or IMP carbapenemases (collectively known as MBLs).
Rationale
Carbapenemase production is an infrequent mechanism of carbapenem resistance among P. aeruginosa isolates in the United States [387, 414]. In contrast, carbapenemases (most commonly KPC or VIM carbapenemases) are identified in a substantial proportion of carbapenem-resistant P. aeruginosa isolates in other regions of the world, including Latin America (approximately 69%), Asia (57%), and Southern Europe (50%) [387, 415-418]. With increasing globalization and international travel, the prevalence of carbapenemase-producing P. aeruginosa in the United States is likely to rise. The clinical relevance of this threat was underscored by a 2022–2023 outbreak of P. aeruginosa, producing both VIM and GES (i.e., Guiana extended-spectrum β-lactamase enzymes), linked to contaminated artificial tears, which resulted in 81 infections across the United States, permanent vision loss in 17% of cases and death in 5% [419-421].
In addition to carbapenemases, other β-lactamase enzymes - such as GES, Vietnamese extended-spectrum β-lactamase (VEB), and Pseudomonas extended resistance (PER) enzymes - remain rare in the United States but may confer elevated MICs to multiple β-lactam agents, including newer β-lactams [19, 422]. Notably, some GES alleles (e.g., GES-5) have carbapenemase activity whereas other alleles (e.g., GES-1) do not [423]. Although emerging molecular technologies can detect blaGES, blaVEB, and blaPER genes in clinical specimens, these assays are infrequently used in routine clinical microbiology practice. In contrast, several FDA-cleared multiplex assays are available for detection of KPC, VIM, IMP, NDM, and OXA-48 carbapenemases, including from blood cultures and respiratory specimens. Consequently, carbapenemase gene results are often available before AST results for newer β-lactam agents, highlighting the importance of understanding how carbapenemase identification should inform antibiotic decision-making.
When blaKPC genes are identified in P. aeruginosa isolates, ceftolozane-tazobactam is not suggested, as tazobactam does not inhibit KPC enzymes. While the in vitro potency of cefiderocol, ceftazidime-avibactam, and imipenem-relebactam against KPC-producing Enterobacterales is well established, data characterizing the activity of these agents against KPC-producing P. aeruginosa isolates are limited. Although avibactam and relebactam inhibit KPC in vitro, a study that included 44 KPC-producing P. aeruginosa isolates found that 21 (48%) were resistant to ceftazidime-avibactam and 32 (75%) were resistant to imipenem-relebactam[412]. The decision between cefiderocol, ceftazidime-avibactam, and imipenem-relebactam for KPC-producing P. aeruginosa infections should be made based on AST results.
When NDM, VIM, or IMP are identified (i.e., MBLs), ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam are not suggested, as none of these β-lactamase inhibitors have activity against MBLs. When carbapenemase testing results are not available for DTR P. aeruginosa isolates, concurrent resistance to ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam should raise suspicion for MBL production, with VIM being the most common carbapenemase produced by P. aeruginosa in the United States [387]. Cefiderocol is the preferred treatment for MBL-producing P. aeruginosa [300, 323, 424], although clinical outcomes data remain limited [324, 425]. Of concern, cefiderocol-resistant MBL-producing P. aeruginosa isolates are being reported [426, 427], leaving no remaining active β-lactam options. Importantly, identification of carbapenemase genes does not obviate the need for susceptibility testing, and AST for preferred agents should still be pursued.
Although aztreonam-avibactam generally is active against MBL-producing Enterobacterales, this combination has limited activity against MBL-producing P. aeruginosa; neither CLSI nor FDA susceptibility breakpoints are available[428, 429]. While avibactam may reduce aztreonam hydrolysis by PDC enzymes, active efflux (e.g., MexAB–OprM) limit aztreonam from achieving adequate intracellular concentrations at its PBP3 target [430]. The addition of ceftazidime to aztreonam-avibactam increases the in vitro activity of this combination against MBL-producing P. aeruginosa [431, 432], but clinical data supporting ceftazidime-avibactam plus aztreonam remain limited to small case series [433-435]. The panel does not suggest aztreonam-avibactam for MBL-producing P. aeruginosa; ceftazidime-avibactam plus aztreonam is suggested only when resistance precludes the use of cefiderocol.
Question 4.5: What is the likelihood of emergence of resistance of DTR P. aeruginosa to newer β-lactam agents when used to treat DTR P. aeruginosa infections?
Suggested approach: Emergence of resistance during therapy is a concern with all β-lactam agents used to treat P. aeruginosa infections. Available data suggest that treatment-emergent resistance occurs in approximately 20% of isolates treated with newer β-lactams.
Rationale
The likelihood of activity of the four β-lactam agents currently available in the United States with activity against DTR P. aeruginosa (i.e., cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam) varies by agent. Among 167 DTR P. aeruginosa isolates collected from 2019-2021 across the United States, susceptibility proportions were 50% for ceftazidime-avibactam, 74% for ceftolozane-tazobactam, and 37% for imipenem-relebactam; cefiderocol was not evaluated [411]. In a separate study of 154 DTR isolates collected from 2020-2023, susceptibility was 99%, 61%, 71%, and 62% for cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, and imipenem-relebactam, respectively [436]. Across surveillance studies, cefiderocol generally has the greatest likelihood of in vitro activity against MDR and DTR P. aeruginosa [424, 436, 437].
As with all antibiotics used for P. aeruginosa infections, treatment with newer β-lactams increases the likelihood that subsequent isolates will no longer be susceptible. The emergence of resistance has been most extensively evaluated for ceftazidime-avibactam and ceftolozane-tazobactam, reflecting their more frequent use in clinical practice relative to cefiderocol and imipenem-relebactam [438].
For ceftazidime-avibactam, resistance most commonly arises through amino acid substitutions in chromosomal PDCs, particularly within or adjacent to the omega loop [439-443]; reduced affinity of PBP3 for ceftazidime has also been occasionally identified [444]. Mechanisms of resistance emerging during ceftolozane-tazobactam therapy closely mirror those observed with ceftazidime-avibactam, consistent with their shared cephalosporin core structure. Although ceftolozane contains R2 side-chain modifications that enhance stability against PDCs and improve PBP binding [214], cross-resistance between ceftazidime-avibactam and ceftolozane-tazobactam exceeds 50% [406, 442, 443]. Emergence of non-susceptibility during ceftazidime-avibactam or ceftolozane-tazobactam therapy has been reported in approximately 24% of DTR P. aeruginosa infections [406, 407, 445].
Cefiderocol is a siderophore-cephalosporin that exploits iron acquisition systems of P. aeruginosa by mimicking iron-binding siderophores, allowing it to enter bacterial cells through TonB-dependent receptors rather than traditional porins [334]. Once in the periplasmic space, cefiderocol inhibits PBPs, particularly PBP3, disrupting cell wall synthesis. Consequently, mutations of components of this pathway can confer cefiderocol resistance as can modifications to PBP3 [446, 447]. Moreover, the absence of a β-lactamase inhibitor renders cefiderocol vulnerable to resistance mechanisms mediated by PDC and other β-lactamase overexpression or structural modifications [446, 448, 449]. Given shared structural features among cephalosporins, increases in cefiderocol MICs have been observed in approximately 15% of P. aeruginosa isolates following exposure to ceftazidime-avibactam or ceftolozane-tazobactam [448, 450]. In contrast, limited data suggest that fewer than 10% of P. aeruginosa isolates develop cefiderocol resistance during treatment [259].
Resistance to imipenem-relebactam most commonly develops through loss or modification of the OprD porin and/or overexpression of efflux pumps such as MexAB-OprM or MexEF-OprN [451, 452]. OprD alterations reduce imipenem uptake, while relebactam - although able to protect imipenem against PDC enzymes - remains susceptible to efflux [451, 452]. Across two clinical trials including 50 patients with P. aeruginosa infections treated with imipenem-relebactam, no emergence of imipenem-relebactam resistance was observed [274, 396]. However, in two observational studies including 46 patients, treatment-emergent imipenem-relebactam non-susceptibility developed in approximately 24% of patients [413, 453].
Although estimates will continue to evolve, emergence of resistance during therapy remains a concern across all four newer β-lactam agents, supporting repeat AST for isolates recovered in culture while on therapy or for those from patients who re-present with suspected DTR P. aeruginosa infection.
Question 4.6: What is the role of combination antibiotic therapy for the treatment of infections caused by DTR P. aeruginosa?
Suggested approach: Combination antibiotic therapy is not suggested for infections caused by DTR P. aeruginosa when in vitro susceptibility to cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, or imipenem-relebactam has been confirmed.
Rationale
Although empiric combination therapy (e.g., addition of tobramycin to a newer β-lactam) may be reasonable to increase the likelihood of initial coverage in patients at risk for DTR P. aeruginosa infection, available data do not support continued combination therapy once susceptibility to a β-lactam agent has been confirmed. Specifically, combination therapy has not been shown to improve clinical outcomes compared with β-lactam monotherapy and is associated with a higher risk of antibiotic-related adverse events[367]. Moreover, clinical data demonstrating that combination therapy prevents the emergence of resistance are lacking.
Clinical trials comparing monotherapy versus combination therapy for the newer β-lactam agents are not available. Observational studies have not identified a survival benefit associated with combination therapy [454, 455]. Considering the known toxicities of aminoglycosides and polymyxins, and the absence of demonstrated clinical benefit, the panel does not suggest routine use of combination therapy for DTR P. aeruginosa infections when an active β-lactam agent is available.
When no β-lactam agent demonstrates in vitro activity, combination therapy with tobramycin (if susceptible) and a newer β-lactam may be considered, preferentially selecting the β-lactam with an MIC closest to its susceptibility breakpoint. For example, if ceftazidime-avibactam and ceftolozane-tazobactam MICs are >128/4 µg/mL and the imipenem-relebactam MIC is 4/4 µg/mL (intermediate), imipenem-relebactam in combination with tobramycin is favored. Data supporting improved outcomes with this strategy are lacking. Notably, aminoglycoside monotherapy is not suggested for DTR P. aeruginosa infections outside of the urinary tract due to suboptimal probabilities of achieving pharmacodynamic exposures associated with bactericidal activity [456, 457].
If tobramycin susceptibility is not demonstrated, polymyxin B may be considered in combination with a newer β-lactam. For infections outside the urinary tract, polymyxin B is preferred over colistin because it is administered in its active form, achieves more reliable plasma concentrations, and may be associated with a lower risk of nephrotoxicity [458-460].
Question 4.7: What is the role of nebulized antibiotics for the treatment of DTR P. aeruginosa pneumonia?
Suggested approach: The panel does not suggest the routine use of nebulized antibiotics for the treatment of pneumonia caused by DTR P. aeruginosa when in vitro susceptibility to an active systemic β-lactam agent has been demonstrated.
Rationale
Three clinical trials have evaluated adjunctive nebulized antibiotic therapy versus placebo in adults with gram-negative pneumonia, with all participants permitted to receive concomitant systemic antibiotics. These studies included nebulized colistin in 100 patients (34% with P. aeruginosa) [461]; nebulized amikacin/fosfomycin in 142 patients (22% with P. aeruginosa) [462]; and nebulized amikacin in 508 patients (32% with P. aeruginosa) [463]. None of these trials demonstrated improvements in clinically meaningful outcomes, including survival, either in the overall study populations or within subgroups infected with drug-resistant pathogens.
Multiple systematic reviews and meta-analyses have further analyzed evidence from clinical trials and observational studies evaluating adjunctive inhaled antibiotic therapy for pneumonia, including infections caused by MDR P. aeruginosa, but not DTR P. aeruginosa [464-467]. None have identified a survival benefit with adjunctive inhaled antibiotics; some have identified modest improvements in clinical response [464-466].
Although PK/PD modeling suggest that aerosolized antibiotics can achieve high epithelial lining fluid concentrations [468], several factors may limit the clinical effectiveness of nebulized antibiotics. These include inadequate penetration into consolidated lung parenchyma and heterogeneous drug distribution within infected airways, which may preclude sustained bactericidal activity [469]. Such limitations likely reflect, in part, the off-label use of parenteral formulations and delivery via nebulization devices (e.g., jet nebulizers) not specifically optimized for pulmonary drug delivery [470, 471]. Accordingly, recommendations from professional societies regarding the use of adjunctive inhaled antibiotics remain inconsistent [472-475].
Given the absence of a survival benefit, the panel does not support the routine use of adjunctive nebulized antibiotics for pneumonia caused by DTR P. aeruginosa. However, selective adjunctive use (e.g. tobramycin, amikacin, colistin methanesulfonate) is reasonable in patients for whom no newer β-lactam agents exhibit in vitro activity against P. aeruginosa and in whom clinical response to systemic therapy is suboptimal. In such circumstances, adverse events such as bronchoconstriction, laryngeal injury, and hypersensitivity pneumonitis should be considered [476, 477].
Section 5: Carbapenem-resistant Acinetobacter baumannii complex (CRAB)
CRAB is a formidable nosocomial pathogen with a remarkable ability to persist in healthcare environments, evade host immune defenses, and acquire diverse AMR mechanisms [478]. For simplicity, this guidance uses the term “CRAB,” recognizing that many clinical microbiology laboratories cannot reliably distinguish A. baumannii from other members of the A. baumannii-calcoaceticus complex[479].
CRAB is most frequently isolated from respiratory tract and wound cultures, where distinguishing colonization from true infection, particularly in mechanically ventilated patients or those with extensive burns, can be challenging. Invasive CRAB infections occur predominantly in critically ill patients with substantial comorbidities, and poor clinical outcomes are often influenced by host factors and severity of illness, complicating attribution to antibiotic therapy alone.
A defining feature of A. baumannii is its extraordinary capacity to accumulate resistance mechanisms, which rapidly eliminates most antibiotic options once carbapenem resistance emerges [480]. Resistance is mediated through multiple, often coexisting mechanisms. These include production of enzymes such as A. baumannii–derived cephalosporinases (ADCs), which inactivate many traditional β-lactams, and OXA-type carbapenemases (e.g., OXA-23, OXA-24/40, OXA-58), which confer resistance to traditional β-lactam antibiotics, including carbapenems [481-484]. Aminoglycoside activity is frequently compromised by aminoglycoside-modifying enzymes or 16S rRNA methyltransferases, often resulting in class-wide resistance [485]. In addition to enzymatic mechanisms, CRAB commonly exhibits reduced outer membrane permeability due to loss or alteration of porins limiting carbapenem entry (e.g., CarO, OmpA) [486]. Moreover, the increased hydrophobicity of the outer membrane contributes to decreased entry of β-lactams and aminoglycosides [487]. Overexpression of intrinsic efflux pumps (e.g., AdeABC, AdeIJK) further contributes to resistance across multiple antibiotic classes, including β-lactams, fluoroquinolones, and tetracycline derivatives [488]. Target site modifications also play an important role; alterations in PBPs (e.g., PBP1a/1b and PBP3) reduce sulbactam activity [489, 490], while mutations in DNA gyrase and topoisomerase IV decrease fluoroquinolone susceptibility [491]. The convergence of extensive multidrug resistance, diagnostic uncertainty, and limited effective therapies contribute to the challenges of managing CRAB infections. This guidance document focuses on the treatment of invasive CRAB infections.
Question 5.1: What is the role of sulbactam-durlobactam for the treatment of invasive CRAB infections?
Suggested approach: Sulbactam-durlobactam, in combination with imipenem or meropenem, is the preferred treatment for invasive CRAB infections.
Rationale
Sulbactam shares the bicyclic β-lactam core of penicillins, with a distinguishing sulfone moiety, rendering it susceptible to hydrolysis by class A (e.g., TEM-1), class C (e.g., ADC-30), and class D (e.g., OXA-23) β-lactamases commonly produced by CRAB isolates [492]. Durlobactam, a diazabicyclooctane β-lactamase inhibitor structurally related to avibactam, inhibits class A, C, and D enzymes but lacks activity against class B enzymes (i.e., MBLs) such as NDMs. By preventing β-lactamase-mediated hydrolysis, durlobactam enables sulbactam to effectively engage PBP1a/1b and PBP3 [493], with surveillance data showing activity against over 95% of CRAB isolates in the United States [494, 495]. Although NDM-producing CRAB isolates remain uncommon in the United States [480, 496], they are increasingly reported in South Asia and the Middle East [497-500].
In a randomized trial including 125 patients with CRAB pneumonia or bloodstream infections, 28-day survival was higher with sulbactam-durlobactam plus imipenem than with colistin plus imipenem (81% [51/63] versus 68% [42/62]) as was clinical cure (62% [39/63] versus 40% [25/62]) [501]. Notably, the comparator regimen (i.e., colistin plus imipenem) is not a preferred or alternative therapy for CRAB. Nonetheless, given the higher survival in the sulbactam-durlobactam arm and given that survival in other CRAB trials frequently is less than 60% [502], these findings support sulbactam-durlobactam as a preferred option for invasive CRAB infections.
Evidence further indicates that adding a carbapenem (imipenem or meropenem) [503] enhances sulbactam-durlobactam activity through complementary PBP binding, with sulbactam targeting PBP1a/1b and PBP3 and imipenem preferentially binding PBP2, while both agents are protected from β-lactamase hydrolysis by durlobactam [504-506]. In vitro, combination therapy with a carbapenem reduces sulbactam MICs by one- to two-fold and achieves >2-log CFU/mL reductions in time-kill assays, activity not observed with sulbactam–durlobactam alone [504, 506, 507]. Although confirmation of the clinical benefit of these in vitro observations are needed, the panelists suggest adding imipenem or meropenem to sulbactam-durlobactam for the treatment of invasive CRAB infections. For patients requiring prolonged durations of therapy (e.g., CRAB osteomyelitis), although data are not available regarding the benefit of continuing dual therapy, it may be reasonable to discontinue the carbapenem component after sustained clinical improvement has been achieved.
Mechanisms of resistance to sulbactam-durlobactam during therapy are incompletely characterized. Available data suggest resistance may arise from combinations of PBP1a/b or PBP3 mutations and/or overexpression of efflux pumps (e.g., AdeIJK) [508-510]. While confirmatory susceptibility testing is suggested, the high likelihood of susceptibility among United States CRAB isolates supports empiric initiation of sulbactam-durlobactam for invasive CRAB infections while awaiting AST results. Clinical data to guide management of sulbactam-durlobactam-resistant CRAB infections are lacking. If resistance to sulbactam-durlobactam (MIC ≥16/4 µg/mL) or an MBL gene (e.g., blaNDM) is identified, the panel prefers non-sulbactam-based regimens (e.g., combinations of cefiderocol, minocycline, polymyxin B, or tigecycline), as sulbactam-based therapy is unlikely to provide meaningful additional benefit, although limited in vitro data suggest sulbactam-durlobactam may enhance cefiderocol activity in these settings [511].
Question 5.2: What is the role of ampicillin-sulbactam for the treatment of invasive CRAB infections?
Suggested approach: If sulbactam-durlobactam is not immediately available, high-dose ampicillin-sulbactam (total daily dose of 9 grams of the sulbactam component) in combination with at least one additional agent (e.g., cefiderocol, minocycline, or polymyxin B) may be used as a temporary bridging therapy for invasive CRAB infections only until sulbactam-durlobactam (in combination with a carbapenem) can be initiated.
Rationale
As described in Question 5.1, sulbactam is a competitive, irreversible β-lactamase inhibitor that, at high exposures, binds and saturates PBP1a/1b and PBP3 of A. baumannii [489, 512]. Sulbactam activity against A. baumannii has been demonstrated across multiple pharmacodynamic investigations [513-515], animal models [516-518], and clinical outcomes studies [502, 519, 520], including infections caused by isolates categorized as non-susceptible by standard susceptibility testing.
Ampicillin-sulbactam is formulated in a fixed 2:1 ratio; for example, a 3-gram dose contains 2 grams of ampicillin and 1 gram of sulbactam. AST for ampicillin-sulbactam is likewise reported in a fixed ratio, permitting estimation of sulbactam MICs. For instance, an ampicillin-sulbactam MIC of 8/4 µg/mL corresponds to a sulbactam MIC of 4 µg/mL, which aligns with the CLSI susceptibility breakpoint for sulbactam (Table 2) [21]. Surveillance data suggest that only approximately 10% of CRAB isolates are susceptible to sulbactam [521, 522]. Unlike sulbactam-durlobactam, ampicillin-sulbactam lacks a β-lactamase inhibitor capable of protecting sulbactam from hydrolysis by the β-lactamases commonly produced by CRAB.
Several studies suggest that high-dose ampicillin-sulbactam (e.g., 9 grams IV every 8 hours administered as a prolonged infusion, corresponding to a total daily sulbactam dose of 9 grams) may partially overcome elevated sulbactam MIC distributions in CRAB [517, 523, 524]. Neutropenic murine lung infection models suggest a total daily sulbactam dose of 4 grams achieves >90% probability of target attainment for isolates with sulbactam MICs ≤4 µg/L (i.e., susceptible), whereas a total daily dose of 9 grams extended coverage to isolates with MICs up to 8 µg/mL (i.e., intermediate) [517, 518].
Standard doses of ampicillin-sulbactam appear adequate for infections caused by sulbactam-susceptible CRAB isolates. However, inaccuracies associated with commonly used AST methods for ampicillin-sulbactam in CRAB - particularly when methods other than reference broth microdilution are employed raise concern that isolates categorized as “susceptible” may in fact be non-susceptible [525, 526]. Given the high mortality associated with invasive CRAB infections, misclassification of susceptibility may lead to suboptimal therapy.
Two meta-analyses encompassing more than 20 observational studies or clinical trials and over 2,000 patients with CRAB infections suggest that sulbactam-containing regimens are associated with improved clinical outcomes compared with alternative therapies, which most often consisted of polymyxin- or tetracycline-based regimens [519, 520]. Many patients included in these analyses were infected with sulbactam-resistant isolates. Both meta-analyses were limited by the predominantly observational nature of included studies, small sample sizes, heterogeneous antibiotic regimens and dosing strategies, and limited differentiation between colonization and infection. Among the five clinical trials evaluating survival in invasive CRAB infections that included sulbactam in one treatment arm [501, 502, 527-529], only one demonstrated a statistically significant survival benefit [530]; however, all trials reported numerically higher survival in the sulbactam-containing arm. Importantly, safety signals have not been identified with high-dose sulbactam across clinical studies.
Taken together, available preclinical and clinical data suggest that standard-dose ampicillin-sulbactam (3 g IV every 6 hours infused over 30 minutes) may be sufficient for infections caused by sulbactam-susceptible CRAB isolates. Nonetheless, due to potential AST misclassification, the absence of significant toxicity with higher doses, and the substantial mortality associated with inadequately treated invasive CRAB infections, the panel favors the use of high-dose ampicillin-sulbactam administered as a prolonged infusion even for isolates reported as sulbactam susceptible (Table 1).
Although clinical evidence demonstrating superior outcomes with combination therapy remains limited, hydrolysis of sulbactam by CRAB isolates is anticipated in the absence of a protective β-lactamase inhibitor. Accordingly, the panel favors combining high-dose ampicillin-sulbactam with a second active agent (e.g., cefiderocol, minocycline, or polymyxin B). Importantly, high-dose ampicillin–sulbactam combined with a second agent should only be used as a bridging option while awaiting initiation of sulbactam-durlobactam in combination with a carbapenem, assuming sulbactam-durlobactam is not immediately available. Sulbactam-durlobactam plus a carbapenem remains preferred for invasive CRAB infections.
Question 5.3: What is the role of cefiderocol therapy for the treatment of invasive CRAB infections?
Suggested approach: Cefiderocol in combination with at least one other agent (i.e., high-dose ampicillin-sulbactam, minocycline, or polymyxin B) is an alternative treatment for invasive CRAB infections.
Rationale
Surveillance data indicate that more than 90% of CRAB isolates demonstrate in vitro susceptibility to cefiderocol [300, 322, 437, 494]. However, although rarely encountered in the United States, NDM-producing CRAB isolates exhibit substantially reduced susceptibility, with only approximately 60% remaining susceptible to cefiderocol [322]. Although the incidence has not been well quantified, the emergence of cefiderocol resistance among CRAB isolates during therapy remains a concern and is most commonly associated with alterations in iron uptake pathways - such as disruption or downregulation of the pirA and piuA genes - as well as overexpression of β-lactamases (e.g., ADCs) [531-534].
Compared with other gram-negative pathogens, A. baumannii generally requires higher cefiderocol PK/PD targets to achieve optimal bacterial killing and animal models of A. baumannii infection have demonstrated variable bactericidal activity with cefiderocol [535-538].
Clinical outcome data for cefiderocol in CRAB infections remain inconclusive. Notably, no clinical trials or observational studies have compared outcomes among patients treated with cefiderocol versus sulbactam-durlobactam. In a randomized clinical trial that included a subgroup of 54 patients with CRAB infections, 28-day survival was 51% (20/39) among patients treated with cefiderocol compared with 82% (14/17) among those receiving alternative regimens, which were predominantly polymyxin-based [259]. In a second randomized clinical trial enrolling 47 patients with CRAB pneumonia, 14-day survival occurred in 78% (18/23) of patients receiving cefiderocol and 83% (20/24) receiving high-dose, extended-infusion meropenem [539]; although limited by small numbers, these results are concerning given that cefiderocol demonstrated outcomes comparable to an agent lacking meaningful activity against CRAB isolates. A third randomized clinical trial included 25 patients with CRAB bacteremia and reported 30-day survival of 55% (6/11) versus 50% (7/14) for cefiderocol and alternative therapy (i.e., mostly combinations of ampicillin-sulbactam and polymyxins), respectively[325].
In contrast, observational data have suggested more favorable outcomes with cefiderocol therapy for CRAB infections. A meta-analysis including one clinical trial and seven observational studies reported higher pooled 30-day survival with cefiderocol-based therapy of 58% (200/345) versus 40% (182/455) with alternative regimens [540]. A second meta-analysis comprising four observational studies similarly identified higher 30-day survival among patients treated with cefiderocol (62% [104/169]) compared with alternative therapies (37% [95/257])[541]. No patients in the alternative therapy arms across included observational studies received sulbactam-durlobactam. Additionally, there was significant heterogeneity across studies. Given the ongoing uncertainty regarding the effectiveness of cefiderocol in clinical trials, the panel suggests reserving cefiderocol as an alternative option for the treatment of invasive CRAB infections, in combination with a second agent, only when resistance precludes the use of sulbactam-durlobactam or as a bridging therapy until sulbactam-durlobactam availability.
Question 5.4: What is the role of minocycline for the treatment of invasive CRAB infections?
Suggested approach: Minocycline in combination with at least one other agent (i.e., high-dose ampicillin-sulbactam, cefiderocol, or polymyxin B) is an alternative treatment for invasive CRAB infections.
Rationale
Minocycline is a tetracycline derivative available in both IV and oral formulations. Applying the revised 2025 CLSI susceptibility breakpoint (≤1 µg/mL), minocycline demonstrates in vitro activity against fewer than 50% of CRAB isolates (Table 2) [542-544]. The frequency of resistance emergence during minocycline therapy is not well described; however, resistance is associated with overexpression of efflux systems such as AdeABC and TetB [545, 546]. Population PK modeling suggests that minocycline dosed at 200 mg every 12 hours provides a high probability of attaining targets associated with bacterial stasis for isolates with MICs up to the susceptible breakpoint of ≤1 µg/mL, but does not reliably attain targets associated with 1-log killing [547]. Minocycline has not been evaluated in clinical trials for CRAB infections. Available evidence is limited to observational studies, which are constrained by small sample sizes, absence of comparator groups, challenges distinguishing colonization from infection, and heterogeneous patient populations [364, 548-550]. Nonetheless, several reports describe favorable clinical outcomes with minocycline-based therapy for CRAB infections.
Tigecycline, another tetracycline derivative, is available only as an IV formulation. Neither CLSI nor FDA susceptibility breakpoints exist for tigecycline against A. baumannii. Clinical outcomes data suggest that “high-dose” tigecycline (200 mg IV loading dose followed by 100 mg IV every 12 hours) yields outcomes comparable to alternative agents for CRAB infections [353, 551, 552] (Table 1). Hollow-fiber infection models further demonstrate dose-dependent activity against CRAB isolates [553]. However, as with minocycline, PK data from critically ill patients suggest reduced efficacy when MICs exceed 1 µg/mL [554-556]. Direct comparative studies between minocycline and tigecycline are lacking; however, given the absence of established susceptibility criteria for tigecycline, minocycline is preferred when a tetracycline derivative is selected.
Omadacycline is available in both IV and oral formulations, but neither CLSI nor FDA susceptibility criteria exist for A. baumannii isolates. A PK/PD analysis suggests activity of omadacycline against CRAB isolates is limited to stasis and requires higher exposures compared to other pathogens[557]; however, a neutropenic murine thigh infection model suggests similar efficacy as tigecycline for CRAB infections [558]. Clinical data are limited [559, 560]. An observational study evaluating 40 patients with CRAB pneumonia suggested similar 28-day survival of 60% (12/20) and 60% (12/20), respectively, when comparing omadacycline and tigecycline [560]. Given limited PK/PD and clinical data, the panel does not suggest omadacycline for the treatment of CRAB infections unless neither minocycline nor tigecycline are available.
Comparative effectiveness data between tetracycline derivatives and sulbactam–durlobactam are not available. Among tetracyclines, the panel suggests minocycline, in combination with a second active agent, as an alternative option for invasive CRAB infections only in settings of resistance to sulbactam-durlobactam or an interim therapy while awaiting access to sulbactam-durlobactam. This suggestion is based on the availability of minocycline susceptibility criteria, PK/PD-informed dosing considerations, and limited but supportive clinical outcomes data. As with other tetracycline derivatives, minocycline exhibits rapid tissue distribution, resulting in relatively low serum and urinary concentrations [61]. Additionally, gastrointestinal intolerance, particularly nausea, occurs in approximately 20-25% of patients, similar to tigecycline [361, 561, 562].
Question 5.5: What is the role of the polymyxin B for the treatment of invasive CRAB infections?
Suggested approach: Polymyxin B in combination with at least one other agent (i.e., high-dose ampicillin-sulbactam, cefiderocol, or minocycline) is an alternative treatment for invasive CRAB infections.
Rationale
Approximately 85% of CRAB isolates have polymyxin MICs of ≤2 µg/mL [563, 564]. There is no CLSI susceptible category for the polymyxins against A. baumannii; rather, A. baumannii isolates with polymyxin MICs of ≤2 µg/mL fall into the intermediate category [21] (Table 2). The benefit of polymyxins is diminished when polymyxin MICs are >2 µg/mL [565]. Notably, polymyxin B has a more favorable PK profile than colistin [244, 473, 565].
As previously stated, in a randomized clinical trial including 125 patients with CRAB pneumonia or bloodstream infections, 28-day survival was lower with colistin plus imipenem (68% [42/62]) versus sulbactam-durlobactam plus imipenem (81% [51/63]) as was clinical cure (40% [25/62]) versus 62% [39/63]) [501]. There are several concerns with polymyxins. First, serum concentrations of polymyxins achieved are highly variable and may be inadequate for effective bactericidal activity [244]. Second, the activity of IV polymyxins in pulmonary epithelial lining fluid is suboptimal and generally does not result in adequate bacterial killing in the lungs [566-568]. Third, survival with colistin monotherapy across six clinical trials enrolling approximately 500 participants was relatively low, ranging from 27-57% across studies [569-574]. It is unclear if trial outcomes would be improved had polymyxin B been administered instead of colistin. Finally, dosages required to treat systemic CRAB infections approach the threshold for nephrotoxicity, making the therapeutic window extremely narrow (i.e., approximately 2 µg/mL may be required to achieve 1-log10 reduction in bacterial growth, which is also the threshold associated with nephrotoxicity [247].
Given the ongoing uncertainty regarding the clinical effectiveness of polymyxin B and its unfavorable toxicity profile, the panel suggests reserving it as an alternative option for the treatment of invasive CRAB infections, in combination with a second agent, only when resistance precludes the use of sulbactam-durlobactam or as interim therapy while awaiting access to sulbactam-durlobactam.
Question 5.6: What is the role of nebulized antibiotics for the treatment of CRAB pneumonia?
Suggested approach: The panel does not suggest the routine use of nebulized antibiotics for the treatment of pneumonia caused by CRAB.
Rationale
Three randomized clinical trials have assessed adjunctive nebulized antibiotic therapy versus placebo in adults with gram-negative pneumonia, with all participants permitted to receive concomitant systemic antibiotics. These trials evaluated nebulized colistin in 100 patients (65% with A. baumannii pneumonia) [461], nebulized amikacin/fosfomycin in 142 patients (20% with A. baumannii) [462], and nebulized amikacin in 508 patients (29% with A. baumannii) [463]. None of these studies demonstrated improvements in survival, either in the overall study populations or in subgroups infected with drug-resistant pathogens.
Several systematic reviews and meta-analyses have subsequently synthesized data from clinical trials and observational studies evaluating adjunctive inhaled antibiotic therapy for pneumonia, including infections caused by CRAB [464-467]. Consistent with individual trial findings, these analyses have not identified a survival benefit associated with adjunctive inhaled antibiotics, although some have reported modest improvements in clinical response [464-466].
While PK/PD modeling suggests that aerosolized antibiotics can achieve high epithelial lining fluid concentrations [468], several factors likely limit their clinical effectiveness. These include suboptimal penetration into consolidated lung parenchyma and heterogeneous drug distribution within infected airways, which may prevent sustained bactericidal activity [469]. Such limitations may be exacerbated by the off-label use of parenteral formulations and delivery via nebulization devices (e.g., jet nebulizers) that are not specifically designed for pulmonary drug delivery [470, 471]. Reflecting these uncertainties, recommendations from professional societies regarding the use of adjunctive inhaled antibiotics for pneumonia are inconsistent [472-475].
In light of the absence of a clear survival benefit, the panel does not support the routine use of adjunctive nebulized antibiotics for pneumonia caused by CRAB. Nonetheless, selective use may be reasonable in patients with documented resistance to sulbactam-durlobactam or when clinical response to systemic therapy is suboptimal. In such cases, the potential for adverse events, including bronchoconstriction, laryngeal injury, and hypersensitivity pneumonitis, should be carefully weighed [476, 477].
Section 6: Stenotrophomonas maltophilia
S. maltophilia is an aerobic, glucose non-fermenting, gram-negative bacillus that is ubiquitous in water environments [575]. Although generally believed to be less pathogenic than many other nosocomial organisms, S. maltophilia produces biofilm and virulence factors that enable colonization or infection in vulnerable hosts, typically during prolonged hospitalization or extensive antibiotic exposure, particularly carbapenem exposure [576-578]. Accumulating evidence suggests that early initiation of therapy with agents with activity against S. maltophilia is critical for optimizing outcomes in patients with invasive S. maltophilia infections [579-581].
S. maltophilia poses several management challenges. First, although S. maltophilia has the potential to cause severe infection, determining whether S. maltophilia represents a colonizing organism or a true pathogen is difficult, particularly in patients with underlying pulmonary conditions such as cystic fibrosis or ventilator dependency. Moreover, S. maltophilia is often recovered as a component of a polymicrobial infection, further complicating decisions on the necessity of targeted S. maltophilia therapy [582]. Importantly, S. maltophilia can be a true pathogen that causes considerable morbidity, particularly in patients with hematologic malignancies if it causes hemorrhagic pneumonia or bacteremia [583-587].
Second, treatment selection is hampered by AMR genes carried by S. maltophilia isolates[588]. Production of L1 MBLs and L2 cephalosporinases render most conventional β-lactams ineffective [589]. S. maltophilia exhibits resistance to aminoglycosides via chromosomal aminoglycoside acetyl transferase enzymes [590]. Furthermore, S. maltophilia can accumulate resistance mechanisms that reduce the activity of antibiotics with expected activity against S. maltophilia. These include multidrug efflux pumps that increase the MICs of TMP-SMX, tetracyclines, and fluoroquinolones, as well as chromosomal Smqnr genes that further reduce the effectiveness of fluoroquinolones [591-593].
Third, a “standard of care” antibiotic regimen for S. maltophilia infections against which to compare the effectiveness of various treatment regimens is not evident. Clinical trials comparing the effectiveness of commonly used agents for S. maltophilia are lacking. Data to prioritize among agents with in vitro activity against S. maltophilia and to determine the additive benefit of combination therapy regimens remain incomplete.
Lastly, S. maltophilia AST determination is problematic. The CLSI has established breakpoints for six agents against S. maltophilia: cefiderocol, chloramphenicol, levofloxacin, minocycline, ticarcillin-clavulanate, and TMP-SMX [21]. However, ticarcillin-clavulanate manufacturing has been discontinued and chloramphenicol is rarely used in the United States due to significant toxicities, leaving four agents for which interpretable antibiotic MIC values can be provided to clinicians. Confidence in MIC interpretive criteria for several of these agents is further undermined by concerns regarding the reproducibility of commonly employed susceptibility testing methods [594, 595], limited PK/PD data to inform breakpoints for most agents, and insufficient data linking MIC data to clinical outcomes. This guidance document focuses on the treatment of invasive S. maltophilia infections.
Question 6.1: What is the role of cefiderocol for the treatment of invasive S. maltophilia infections?
Suggested approach: Cefiderocol, as monotherapy, is the preferred treatment for invasive S. maltophilia infections, acknowledging this preference is largely based on data derived from neutropenic animal infection models and not clinical outcomes studies.
Rationale
Surveillance studies consistently demonstrate that S. maltophilia susceptibility to cefiderocol approaches 100%, including among isolates resistant to other commonly used agents [45, 322, 596-599]. Reports of cefiderocol resistance (i.e., MICs ≥2 µg/mL) remain rare [403, 599, 600]. Multiple AMR markers may contribute to increasing cefiderocol MICs; a prominent mechanism is mutations in the iron transport system (e.g., tonB) [599].
Multiple neutropenic thigh and lung infection models suggest cefiderocol has potent activity against S. maltophilia and indicate concordance between in vitro susceptibility and in vivo efficacy using human-simulated dosing regimens [535, 601-603]. Modeling indicates that patients treated with cefiderocol have a >90% probability of achieving PK/PD exposure targets that correlate with bactericidal activity in animal models [604]. As one example, in a neutropenic rabbit pneumonia model, cefiderocol eradicated S. maltophilia from lung tissue, whereas TMP-SMX was unable to do so, leaving a residual bacterial burden [603]. Survival was substantially higher among cefiderocol-treated rabbits (88% [7/8]) compared with those receiving TMP-SMX (25% [2/8]); no untreated animals survived.
Clinical data regarding the use of cefiderocol for S. maltophilia infections remain limited, with survival reported in approximately 70% of patients in observational cohorts [403, 605-607]. Comparisons between cefiderocol and alternative regimens are challenging because of substantial heterogeneity across studies and the absence of direct comparative data. Notably, a meta-analysis of 14 studies including 663 patients treated with alternative agents for S. maltophilia infections (e.g., TMP-SMX, fluoroquinolones) similarly reported survival in approximately 70% of patients [608]. Clinical trial data are restricted to small subgroup analyses. In one trial, only five patients with S. maltophilia infections were assigned to the cefiderocol arm, of whom one (20%) survived, precluding meaningful comparisons with alternative therapy [259]. In a second trial, 30-day survival was 60% (3/5) among patients receiving cefiderocol, compared with 100% (3/3) among those receiving alternative therapy, which consisted of levofloxacin-based regimens [325].
Notwithstanding these limited, and in some cases unfavorable, clinical data, the panel suggests cefiderocol as a preferred therapy for S. maltophilia infections based on its high likelihood of in vitro activity against S. maltophilia isolates and its consistent bactericidal activity demonstrated in animal models. There are insufficient data to indicate improved clinical outcomes with the use of cefiderocol as a component of combination therapy.
Question 6.2: What is the role of aztreonam-avibactam for the treatment of invasive S. maltophilia infections?
Suggested approach: Aztreonam-avibactam, preferably in combination with a second agent, is an alternative treatment option for invasive S. maltophilia infections.
Rationale
The L1 metallo-β-lactamases produced by S. maltophilia hydrolyze all β-lactams except aztreonam; whereas, the L2 cephalosporinases hydrolyzes aztreonam, along with other β-lactam agents [589]. Avibactam, however, can inhibit the activity of L2 cephalosporinases [609]. Consequently, the combination of aztreonam-avibactam enables aztreonam to reach and bind to PBP3, its primary target, in S. maltophilia [610, 611].
Although CLSI and FDA susceptibility breakpoints for aztreonam-avibactam against S. maltophilia have not been established as of 2026, surveillance data indicate that >90% of S. maltophilia isolates have MICs ≤4/4 µg/mL, the susceptibility breakpoint used for Enterobacterales (Table 2) [612-615]. Resistance to aztreonam-avibactam in S. maltophilia may result from overexpression of the L1 and/or L2 β-lactamase, along with upregulation of the Sme multidrug efflux pumps [609, 616].
Regarding PK/PD data, in a neutropenic murine thigh infection model assessing 27 S. maltophilia isolates across a range of aztreonam-avibactam MICs, human-simulated Enterobacterales dosing achieved at least a 1-log₁₀ CFU reduction in 72% mice infected with isolates with MICs ≤4/4 µg/mL [617]. However, the pharmacodynamic target required for aztreonam-avibactam to achieve 1-log killing against S. maltophilia has not been defined, complicating interpretation of these animal data and precluding Monte Carlo simulations to estimate the probability of target attainment in humans.
Clinical data evaluating aztreonam-avibactam for S. maltophilia infections are sparse. Several case reports describe favorable outcomes [618-621]. Subgroup analyses from two clinical trials evaluating aztreonam-avibactam included four patients with S. maltophilia infections, all of whom were randomized to receive aztreonam–avibactam [259, 310]. Clinical outcomes were favorable in one patient, indeterminate in one patient, and unfavorable in two patients, thereby limiting meaningful interpretation of efficacy in this population. Given the limited PK/PD and clinical data, the panel suggests use of aztreonam-avibactam as part of combination therapy, with transition to monotherapy considered only after clear and sustained clinical improvement and confirmation of in vitro susceptibility.
The combination of ceftazidime–avibactam plus aztreonam provides similar activity as aztreonam-avibactam based on mechanistically-informed pharmacodynamic modeling studies [622], although the administration of a single agent (i.e., aztreonam-avibactam) is more convenient [623]. In settings where aztreonam-avibactam is not available, ceftazidime-avibactam plus aztreonam is a reasonable alternative. Practical strategies for administering ceftazidime-avibactam plus aztreonam [315-317] are summarized in Table 1 and the Supplemental Material. Notably, the combination of ceftazidime-avibactam and aztreonam has similar limitations in available PK/PD and clinical outcomes data for S. maltophilia as aztreonam-avibactam.
Question 6.3: What is the role of levofloxacin for the treatment of invasive S. maltophilia infections?
Suggested approach: Levofloxacin, as a component of combination therapy, is an alternative treatment option for invasive S. maltophilia infections.
Rationale
Surveillance data from the United States demonstrate approximately 90% of S. maltophilia isolates are susceptible to levofloxacin (i.e., MICs ≤2 µg/mL) [612, 624]. Emergence of resistance during levofloxacin therapy appears to occur in approximately 20% of cases [625-628]. Resistance to levofloxacin is most commonly mediated by mutations in Smqnr that interfere with fluoroquinolone binding to gyrase and topoisomerase and overexpression of Sme multidrug efflux pumps, both of which may emerge under levofloxacin treatment pressure [591, 629-631].
PK/PD investigations suggest that levofloxacin frequently does not achieve sustained bacterial suppression or PK/PD targets associated with bacterial killing against S. maltophilia [632-635]. Levofloxacin dosed at 750 mg IV every 24 hours had approximately a 50% probability of achieving exposure targets associated with bacterial stasis in a neutropenic murine thigh infection model when the isolate has an MIC value of 2 µg/mL (the CLSI susceptible breakpoint), and an approximately 27% probability of achieving targets associated with a ≥1-log reduction in bacterial load [632]. In a murine pneumonia model, levofloxacin improved survival relative to placebo (50% versus 0%), though eradication of infection was not consistently achieved [636].
Clinical trial data evaluating levofloxacin for S. maltophilia infections are lacking. Observational studies are constrained by small sample sizes, heterogeneous infection sites, potential misclassification of colonization versus infection, frequent use of concomitant antibiotics, and inconsistent dosing strategies [580, 608, 626, 627, 637-644]. Across studies, no single agent, levofloxacin, minocycline, or trimethoprim-sulfamethoxazole, has been definitively associated with more favorable patient outcomes. Combination therapy is frequently employed in published cohorts; however, studies have not clearly demonstrated improved outcomes with combinations of levofloxacin, minocycline, or TMP-SMX compared with monotherapy with these agents [580, 645, 646].
Given the variable baseline susceptibility, risk of resistance emergence during therapy, limited PK/PD support for bactericidal activity, and difficult to interpret clinical outcomes data, the panel suggests levofloxacin as a component of combination therapy for invasive S. maltophilia infections. Levofloxacin-associated toxicities include tendinopathy, QT prolongation, dysglycemia, increased risk of C. difficile infections, and central nervous system effects [647]. Oral levofloxacin achieves high bioavailability with systemic exposures comparable to IV administration [648]. Transition to levofloxacin monotherapy should be considered only after clear and sustained clinical improvement has been achieved and susceptibility is confirmed.
Question 6.4: What is the role of minocycline for the treatment of invasive S. maltophilia infections?
Suggested approach: Minocycline, as a component of combination therapy, is an alternative treatment option for invasive S. maltophilia infections.
Rationale
Among tetracycline derivatives, minocycline has the most favorable pre-clinical data supporting its activity for S. maltophilia infections. Surveillance data from the United States demonstrate in vitro susceptibility to minocycline in approximately 90% of isolates (MIC ≤1 µg/mL)[612]. S. maltophilia resistance to minocycline primarily involves overexpression of Sme multidrug efflux pumps [649]. CLSI susceptibility breakpoints are available for minocycline against S. maltophilia[21] (Table 2), whereas neither CLSI nor FDA breakpoints exist for other tetracycline derivatives.
The strongest evidence supporting minocycline derives from PK/PD investigations[635, 650, 651]. Minocycline dosed at 200 mg IV every 12 hours has approximately a >90% probability of achieving exposure targets associated with bacterial stasis in a neutropenic murine thigh infection model when the isolate has an MIC value of 1 µg/mL (the CLSI susceptible breakpoint), and approximately a 50% probability of achieving targets associated with a ≥1-log reduction in bacterial burden [651]. Similar investigations have not been conducted for other tetracycline-derivatives.
As with levofloxacin (Question 6.3), clinical trials evaluating minocycline for S. maltophilia are lacking and observational data have not clearly favored levofloxacin, minocycline, or TMP-SMX over each other [641, 642, 652-654]. Cohort studies have not clearly demonstrated improved outcomes with combinations of levofloxacin, minocycline, or TMP-SMX compared with monotherapy with these agents [580, 645, 646].
The panel suggests minocycline as a component of combination therapy for invasive S. maltophilia infections, given the limitations of the PK/PD and clinical data. This suggestion is further informed by minocycline’s relatively low sustained serum concentrations [61], which raise concern regarding its reliability as monotherapy for invasive disease involving the bloodstream. Transitioning to minocycline as monotherapy should only be considered after clear and sustained clinical improvement is observed. The panel considers IV and oral minocycline interchangeable, as oral administration achieves approximately 95% bioavailability and comparable serum concentrations, steady-state trough levels, and elimination half-lives relative to IV dosing [562]. The most common adverse events associated with minocycline include gastrointestinal symptoms, vestibular effects, and skin reactions [561, 562].
Given the availability of susceptibility criteria and well-characterized PD targets derived from animal models, minocycline is preferred over tigecycline for S. maltophilia. In contrast, data supporting the use of eravacycline or omadacycline for S. maltophilia infections are sparse or unfavorable [655, 656], and their use is not suggested.
Question 6.5: What is the role of TMP-SMX for the treatment of invasive S. maltophilia infections?
Suggested approach: TMP-SMX, as a component of combination therapy, is an alternative treatment option for invasive S. maltophilia infections.
Rationale
Surveillance data from the United States demonstrate in vitro susceptibility of S. maltophilia to TMP-SMX in more than 90% of isolates (MIC ≤2/38 µg/mL) [612, 657]. When resistance occurs, it is commonly mediated by overexpression of multidrug efflux pumps and acquisition of sul and dfrA genes [593, 658, 659].
Despite its extensive historical use, PK/PD investigations consistently demonstrate that TMP-SMX lacks bactericidal activity against S. maltophilia, even when administered at high doses and against isolates with low TMP MICs [596, 650, 660-662]. Across multiple in vitro and PK/PD modeling studies, TMP-SMX achieves, at best, bacterial stasis, with enhanced activity observed when used in combination regimens [650, 661]. A neutropenic rabbit pneumonia model of S. maltophilia, demonstrated that TMP-SMX reduced bacterial burden but failed to eradicate infection and was associated with inferior survival compared with cefiderocol (25% [2/8] versus 88% [7/8], respectively) [603], although the TMP-SMX exposures in these rabbits is unknown.
Clinical trial data evaluating TMP-SMX for S. maltophilia infections are lacking. Available evidence is derived from observational studies, which have yielded no clear consensus regarding the relative effectiveness of TMP-SMX compared with alternative agents such as levofloxacin or minocycline [641, 642, 652-654]. These analyses are limited by heterogeneous infection syndromes, small sample sizes, frequent concomitant antibiotic use, and/or challenges distinguishing colonization from true infection. Whether TMP-SMX is associated with improved outcomes when used as combination therapy compared with monotherapy remains unclear [580, 645, 646].
Despite the absence of consistent evidence demonstrating improved clinical outcomes with TMP-SMX-based combination therapy, the panel suggests TMP-SMX only as a component of combination therapy for invasive S. maltophilia infections, given the limitations of available PK/PD and clinical outcomes data. TMP-SMX is associated with a well-recognized toxicity profile, including hypersensitivity reactions, hematologic abnormalities, gastrointestinal intolerance, hepatotoxicity, renal dysfunction, and electrolyte disturbances, which warrant close monitoring [663]. Oral TMP-SMX achieves essentially complete bioavailability with systemic exposure equivalent to IV administration [664]. Transition to TMP-SMX monotherapy should be considered only after clear and sustained clinical improvement has been achieved.
Question 6.6: What is the role of ceftazidime for the treatment of invasive S. maltophilia infections?
Suggested approach: Ceftazidime is not a suggested treatment for S. maltophilia infections due to the presence of β-lactamase genes intrinsic to S. maltophilia that are expected to render ceftazidime inactive.
Rationale
The panel does not suggest ceftazidime for the treatment of S. maltophilia infections, as L1 and L2 β-lactamases produced by S. maltophilia are expected to render it ineffective. Pre-clinical models suggest ceftazidime is unable to substantially prevent S. maltophilia growth [650]. Comparative effectiveness studies evaluating the role of ceftazidime against S. maltophilia infections are virtually non-existent. As of 2024, neither the CLSI nor the FDA no longer have susceptibility breakpoints for ceftazidime against S. maltophilia [21].
Conclusions
The field of AMR is dynamic and rapidly evolving, and the treatment of AMR infections will continue to challenge clinicians. As newer antibiotics against AMR pathogens are incorporated into clinical practice, we are learning more about their effectiveness and propensity to resistance. This treatment guidance will be updated periodically.
Notes
Acknowledgement
The panel would like to acknowledge selected reviewers for providing constructive feedback on the draft manuscript: Priya Nori, Marisa Holubar, and Ahmed Abdul Azim for their contributions as external reviewers. The panel would also like to acknowledge the contributions of Standards and Practice Guidelines Subcommittee primary reviewers Nicolás Cortés-Penfield and Majdi Al Hasan.
Conflict of Interest Summary
The following list includes what has been reported to IDSA. To provide thorough transparency, IDSA requires full disclosure of all relationships, regardless of relevancy to the guidance topic. Evaluation of such relationships as potential conflicts of interest is determined by a review process which includes assessment by the Board of Directors liaison to the Standards and Practice Guidelines Committee and, if necessary, the Conflicts of Interest and Ethics Committee. The assessment of disclosed relationships for possible conflicts of interests is based on the relative weight of the financial relationship (i.e., monetary amount) and the relevance of the relationship (i.e., the degree to which an association might reasonably be interpreted by an independent observer as related to the topic or recommendation of consideration). IDSA requests panel members to disclose activities and financial relationships/investments related to consultant/advisory roles, promotional speakers bureau, stocks/bonds, honoraria, expert testimony, ownership interest, research grants, organizational benefits, intellectual property, other numeration, activities with other organizations, and relevant financial interest of family members. Readers of this guidance should be mindful of this when the list of disclosures is reviewed.
P.D.T. reports no disclosures. E.L.H. served as a scientific consultant for Lexi-Comp; serves as an associate editor for the Clinical Infectious Diseases journal; receives research funding from the Maryland Department of Health. J.J. has served as a scientific advisor for bioMérieux, Gilead Sciences, and Shionogi; received research funding from the Society of Infectious Diseases Pharmacists; serves as a host/producer of podcasts for the Society of Infectious Diseases Pharmacists; received honoraria from Clinical Care Options and Haymarket Medical Education; owned stock in Vaxart. A.J.M. reports no current industry relationships. She receives research funding from the National Institute of Allergy and Infectious Diseases, the Centers for Disease Control and Prevention, and the Food and Drug Administration, and serves as a volunteer for the Clinical and Laboratory Standards Institute. She previously served as a scientific advisor to Cepheid, Day Zero Diagnostics, bioMérieux, Merck, Shionogi, Qpex Biopharma, Accelerate Diagnostics, VenatoRX and OpGen. M.J.S. receives research funding from Merck, bioMérieux, SNIPRBiome, Hardy Diagnostics, and Melinta Therapeutics; has received consulting fees from Beckman Coulter Diagnostics; has received remuneration from AbbVie for serving on a Data and Safety Monitoring Board; has received consulting fees from Shionogi and has served on a Data and Safety Monitoring Board for Spero Therapeutics. R.A.B. receives research funding from National Institute of Allergy and Infectious Diseases, Centers for Disease Control and Prevention, Veterans Health Administration Merit Award; serves as a clinical scientist investigator for Venatorx Pharmaceuticals; received research funding from Shionogi, Merck, Entasis Therapeutics, Wockhardt, Allecra Therapeutics, AstraZeneca, Harrington Family Foundation, Tetraphase Pharmaceuticals, Steris, National Institute of Allergy and Infectious Diseases, Veterans Health Administration Merit Award, Melinta Therapeutics, NIH and VA, VenatoRx; received an honorarium from Unilab.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References
For a complete list of references, please click here.
Supplemental Material
Publication Disclaimer
© IDSA 2026. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, transmitted, used for text and data mining, or used for training artificial intelligence, in any form or by any means, without the prior permission in writing, or as expressly permitted by law, by license or under terms agreed with the appropriate reprographics rights organization. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through the Oxford University Press RightsLink service via the Permissions link for this paper in Clinical Infectious Diseases. For further information please contact journals.permissions@oup.com.