 In 2016, my sister Dr. Karla V. Saldana shared her decision to pursue a PhD at ETH Zurich, a university in Switzerland. She was focusing on artificial intelligence research. This news left me with mixed feelings of happiness and worry. I was happy because completing a PhD had always been my sister’s dream. However, I was worried because I couldn’t — and still can’t — fully comprehend the impact of these technologies and their influence on the world.
In 2016, my sister Dr. Karla V. Saldana shared her decision to pursue a PhD at ETH Zurich, a university in Switzerland. She was focusing on artificial intelligence research. This news left me with mixed feelings of happiness and worry. I was happy because completing a PhD had always been my sister’s dream. However, I was worried because I couldn’t — and still can’t — fully comprehend the impact of these technologies and their influence on the world.
As an infectious diseases physician in the Southern U.S., I’ve worked in health departments at both state and local levels. I have closely collaborated with public health professionals, including HIV epidemiologists, disease intervention specialists, program managers, linkage coordinators and community educators. Unfortunately, the South is experiencing severe understaffing in its public health workforce. This understaffing has been worsened by the COVID-19 pandemic, resulting in high turnover rates and burnout, which in turn affects the effectiveness of crucial programs and interventions. And let us not forget that the Southern region reported over half of the new HIV diagnoses in the U.S. in 2021.
In Georgia, like in many jurisdictions across the nation, disease intervention specialists are tasked with conducting contact tracing for reportable diseases like HIV and syphilis. However, there are not enough of these specialists to cover all reportable diseases, such as gonorrhea and chlamydia, at least not in the Peach State. For the most part, these diseases are directly reported to the health department by laboratories and providers. Disease intervention specialists then conduct interviews with the goal of referring clients and their partners to appropriate medical and social services. You can imagine the number of HIV and sexually transmitted infection cases in our state is overwhelmingly high, and the burden takes a toll on our understaffed workforce.
After one of the worst earthquakes to hit Ecuador, our home country, in 2016, Karla decided to focus her PhD on “AI for the social good.” In this context, “social good” meant “actions or initiatives that benefit the general welfare and well-being of society, fostering positive outcomes for individuals, communities or the environment.” By combining artificial and human intelligence, Karla trained AI models with multimodal “big data” from natural disasters around the world to predict potential outcomes or assess the impact of tailored interventions in response to catastrophes. These AI models could then be used by political leaders and other stakeholders to mitigate vulnerability to natural disasters. While listening to her thesis dissertation, I thought of the many ways these technologies could be applied to our public health efforts, particularly in the South.
I care for people with HIV at the largest HIV clinic in the country, the Ponce de Leon Center, which serves over 6,000 people with HIV annually. I have heard one too many times “I wish I had known about PrEP sooner,” “I didn't even know PrEP existed,” or “I thought I wasn’t eligible for PrEP.” Furthermore, we far too often see patients admitted to the Special Immunology Service at Grady Memorial Hospital with complications of delayed HIV diagnosis. The question is, what if AI could help us analyze public health data, such as reportable STI cases, and help make predictions about whom our public health workforce should prioritize for HIV testing or referrals to PrEP?
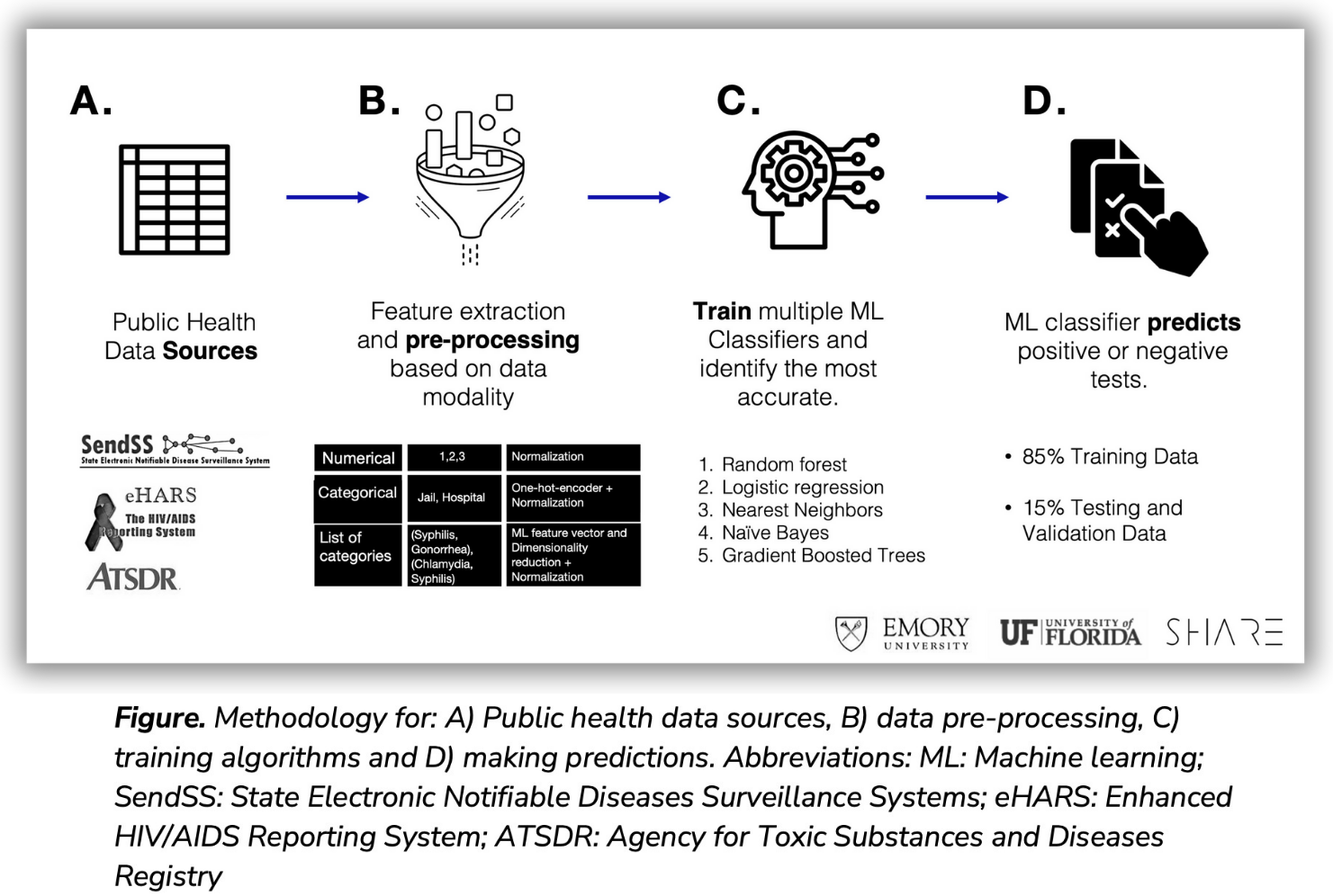
My sister is now a professor at the University of Florida, focusing on AI research. Last year, we partnered with the Georgia Department of Public Health, the Fulton County Board of Health, the University of Florida, and Emory University to develop a machine learning model using de-identified reportable STI data from Fulton County from 2010 to 2021. We matched reportable STI cases to known HIV status through the national HIV database (eHARS) and incorporated social vulnerability indexes via census tract. We trained several machine learning algorithms to learn predictive features of HIV incidence, such as the “X” number of STIs, a diagnosis interval, age at diagnosis, race/ethnicity, and diagnosing providers while using numerical, categorical and even complex combinations of data in arrays (Figure). Our model achieved 80% accuracy in predicting HIV among both males and females. We reported our work and results in a recent article published in Clinical Infectious Diseases. These models use datasets readily available to public health workers, and if validated and collected prospectively, could assist public health workers in making tailored recommendations for HIV testing and prevention for individuals in most need.
There are several limitations to our approach, including reliance on historical data completeness and prediction limited to individuals with a reportable STI, which excludes the general population. Additionally, missing data regarding gender identity and census tracts provide opportunities for enhancement in data collection. Furthermore, the “black box” nature of the algorithm’s feature explainability due to the complexity of multi-modal data analysis means that, at this point, we know it predicts HIV and the most influential features, but we do not fully understand the combinations of features and the granular degree of influence.
We encourage further research to focus on enhancing the explainability of these tools so that policymakers and stakeholders, particularly in the community, can make informed decisions based on these predictive models. At present, no data exist to inform the implementation of these tools into public health practice. Academia, public health professionals, data scientists and the community should continue to collaborate to ensure these tools are implemented in a privacy-preserving way, prioritizing autonomy and intentionally addressing potential biases. They should consider the full spectrum of ethical concerns arising from integrating these tools, ensuring the highest acceptability and feasibility. I do not foresee the implementation of these tools in public health this year or even in the next five. Major improvements in reducing HIV stigma, including the abolition of HIV criminalization nationwide, would need to occur before that. But one can dream, right?

