
CMS Releases 2023 Medicare Physician Fee Schedule Proposed Rule
On July 7, the Centers for Medicare and Medicaid Services (CMS) released its calendar year (CY) 2023 Medicare Physician Fee Schedule (MPFS) proposed rule.
IDSA will continue to share additional information about the proposed rule and will call on the membership to help us advocate to CMS and Congress. Please let us know how the proposed changes may impact you and your ability to recruit and retain ID physicians by emaling clinicalaffairs@idsociety.org. Your voices help inform and strengthen our advocacy.
Please see the key takeaways from the CY 2023 MPFS Proposed Rule resource for additional information.
CMS Reopens the MIPS Extreme and Uncontrollable Circumstances Application for the 2021 MIPS Performance Year in Response to COVID-19
CMS continues to offer flexibilities to provide relief to clinicians responding to the COVID-19 public health emergency. CMS applied the Merit-based Incentive Payment System (MIPS) automatic extreme and uncontrollable circumstances (EUC) policy to all individual MIPS eligible clinicians for the 2021 performance period.
CMS has also reopened the MIPS EUC application for groups, virtual groups, and Alternative Payment Model (APM) Entities through March 31, 2022, at 8 p.m. ET. (Because of the automatic EUC policy, you don’t need to submit an application for individual clinicians.) Please note that applications received between now and March 31, 2022, won’t override previously submitted data for groups and virtual groups.
MIPS EUC applications citing COVID-19 as the triggering event can be submitted until Thursday, March 31, 2022, at 8 p.m. ET.
For more information, please see the CMS Notice for the MIPS Extreme and Uncontrollable Circumstances Application for the 2021 MIPS Performance Year in Response to COVID-19.
Quality Payment Program (as Required by MACRA)
The Centers for Medicare & Medicaid Services (CMS) began the Quality Payment Program (QPP) on January 1, 2017. The QPP fulfills the mandate of the Medicare Access and CHIP Reauthorization Act (MACRA) to implement an incentive program that rewards Medicare-participating clinicians for high quality, cost efficient, value-based care. The QPP comprises two tracks: the Merit-Based Incentive Payment System (MIPS) and the Advanced Alternative Payment Models (APMs). ID physicians may choose which track to participate in based on practice size, location, or patient population.
Most ID physicians will participate in the MIPS. For information on your MIPS eligibility, enter your 10-digit National Provider Identifier (NPI) into the CMS QPP Participation Status tool.
CMS updates the Quality Payment Program and physician payment formulas annually, typically through issuing first a proposed rule, on which it receives public comment, and then a final rule. IDSA continually submits comment letters to CMS on the proposed and final QPP/ Physician fee schedule rules advcoating on behalf of our members.
The Merit-Based Incentive Payment System (MIPS) is a performance-based payment program for clinicians who bill under Medicare Part B and meet the minimum volume threshold requirements implemented by CMS. Clinicians participating in MIPS are evaluated based on four separate categories:
- Quality: Clinicians must select and report on quality measures that evaluate care processes and patient outcomes.
- Improvement Activities: Activities or programs that may improve clinical practice or care delivery, and that will likely result in improved patient outcomes. Clinicians must select at least two from a list updated annually by CMS.
- Promoting Interoperability: Measures of effective electronic health record technology. The use of Certified Electronic health record technology (CEHRT) is required.
- Cost: CMS scores clinicians on multiple cost measures, based on data already submitted through the Medicare administrative claims process for an entire performance year.
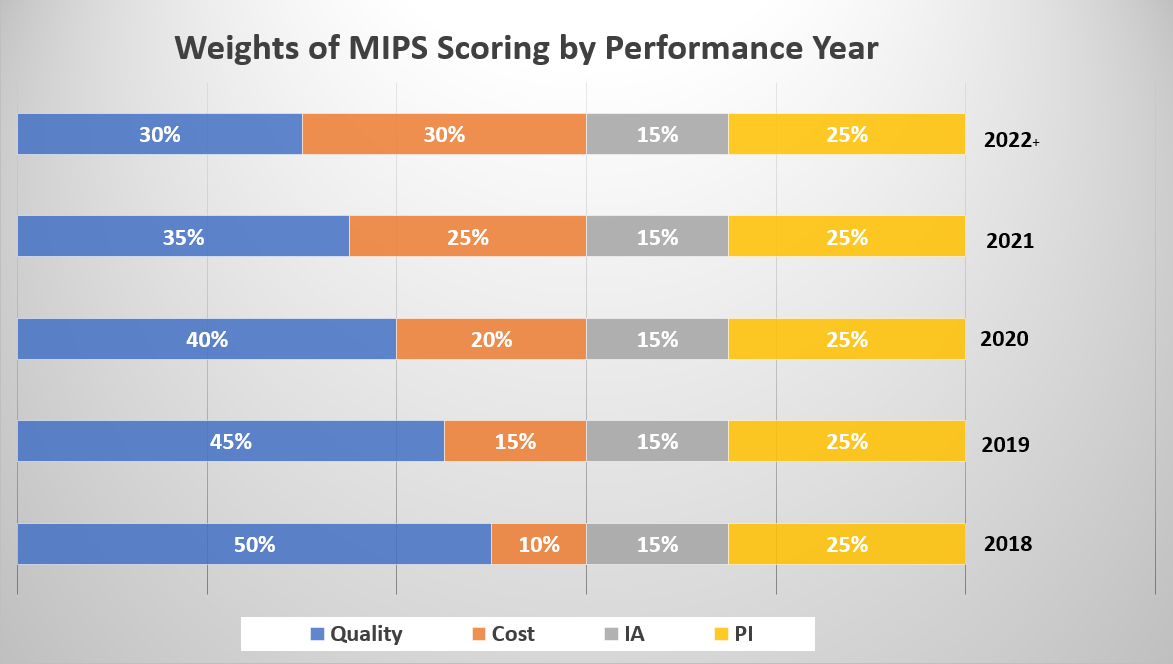
Data for MIPS can be reported at the individual clinician or group practice level. CMS combines performance in each of the four categories to create a composite score to assess overall performance and determine the applicable payment adjustment. There is a two-year lag between the year for which the data are collected—the performance year—and the payment impact (i.e., quality scores collected in performance year 2018 will affect payment in 2020). See the chart below to determine the relative weighting of each category by performance year.
CMS will report on the public Physician Compare website the clinician or group's scores for each category, as well as the final score.
IDSA is aware of the lack of applicable quality measures to the ID physician and has voiced concerns to CMS regarding this troubling issue. IDSA is currently exploring initiatives to address the inappropriate evaluation of ID physicians. IDSA suggests to report on the following measures, depending on where the physician sees patients:
- Measure #110: Preventive Care and Screening Influenza Immunization
- Measure #111: Pneumococcal Vaccination Status for Older Adults
- Measure #128: Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan
- *Measure #130: Documentation of Current Medications in the Medical Record
- Measure #226: Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
- Measure #474: Zoster (Shingles) Vaccination
- Measure #475: HIV Screening
*Indicates high-priority measures
For more details, please use the CMS QPP explore quality-measures tool.
Clinical Practice Improvement Activities
As a part of the MIPS, CMS will also measure the use and reporting of clinical practice improvement activities, which is a new quality measurement category. Improvement activities are activities (such as expanded practice access) or programs (such as antibiotic stewardship) that may improve clinical practice or care delivery and that will likely result in improved outcomes.
Under the new MIPS program, providers can chose from a list of 90+ improvement activities (IAs) in order to meet the requirements of the improvement activity category. IDSA has prepared a list of improvement activities that ID physicians may wish to report. For the first year of the program, in order to avoid a penalty, a provider only needs to report and attest to one improvement activity. IDSA encourages physicians to review the entire list of improvement activities from the Quality Payment Program website.
Providers will need to attest that an improvement activity was performed. CMS has stated that while they’re not requiring physicians to submit any documentation to prove an IA was completed, physicians are encouraged to retain medical records or any other data used to support/determine the completion of the activity for up to 10 years following the performance period.
Example of MIPS Clinical Practice Improvement Activities
- Patient Safety and Practice Assessment: Implementation of an antibiotic stewardship program that measures the appropriate use of antibiotics for several different conditions (URI Rx in children, diagnosis of pharyngitis, Bronchitis Rx in adults) according to clinical guidelines for diagnostics and therapeutics
- Expanded Practice Access: Use of telehealth services and analysis of data for quality improvement, such as participation in remote specialty care consults, or teleaudiology pilots that assess ability to still deliver quality care to patients.
- Emergency Response and Preparedness: Participation in Disaster Medical Assistance Teams, or Community Emergency Responder Teams. MIPS eligible clinicians and MIPS eligible clinician groups must be registered for a minimum of 6 months as a volunteer for disaster or emergency response.
- Population Management: Manage medications to maximize efficiency, effectiveness and safety that could include one or more of the following: Reconcile and coordinate medications and provide medication management across transitions of care settings and eligible clinicians or groups; Integrate a pharmacist into the care team; and/or conduct periodic, structured medication reviews.
- Population Management: Participation in research that identifies interventions, tools or processes that can improve a targeted patient population.
- Population Management: Participation in a QCDR, clinical data registries, or other registries run by other government agencies such as FDA, or private entities such as a hospital or medical or surgical society. Activity must include use of QCDR data for quality improvement (e.g., comparative analysis across specific patient populations for adverse outcomes after an outpatient surgical procedure and corrective steps to address adverse outcome).
Additional Resources
The CMS QPP Experience Report provides a comprehensive representation of the overall clinician experience during QPP performance years with the latest available data to help healthcare professionals understand trends in QPP performance and reporting. Additionally, the QPP Experience Report Public Use Files (PUF) provide further details on QPP participation data.
If you have questions or need assistance with MIPS reporting please contact the Quality Payment Program Service Center.
The help desk is available Monday – Friday; 8:00 AM–8:00 PM ET:
Phone: 1-866-288-8292 TTY: 1-877-715-6222 Email: QPP@cms.hhs.gov
Facility-based measurement offers MIPS eligible clinicians and groups the opportunity to receive scores in the MIPS quality and cost performance categories based on the FY 2022 score for the Hospital Value-Based Purchasing (VBP) Program earned by their assigned facility.
Individual MIPS eligible clinicians qualify for facility-based measurement in the 2021 MIPS performance period when they:
- Billed at least 75% of their covered professional services in a hospital setting (inpatient hospital (Place of Service (POS)=21), oncampus outpatient hospital (POS=22), or emergency room (POS=23)) between October 1, 2019 and September 30, 2020;
- Billed at least one service in an inpatient hospital or emergency room between October 1, 2019 and September 30, 2020; and
- Can be assigned to a facility with a FY 2022 Hospital VBP Program score. (Note that we won’t know if a facility has a FY 2022 score until Fall 2021 at the earliest.)
Groups qualify for facility-based measurement in the 2021 MIPS performance period when:
- More than 75% of the clinicians in the practice qualify for facility-based measurement as individuals
For more information on MIPS facility-based measurement and how to check if you qualify, please review the 2021 Facility-Based Quick Start Guide.
Alternative Payment Models (APMs)
Alternative Payment Models are arrangements that reward participants for providing high-quality cost-effective care. Alternative Payment Models can apply to a specific condition, care episode, or population, and typically rely on care coordination and integration to achieve better results for their patients. CMS designates two kinds of Alternative Payment Models within the Quality Payment Program:
- MIPS APMs: These models include MIPS-eligible clinicians and provide financial incentives for performance on cost, utilization, and/or quality measures at either the participating clinician or APM entity level. Physicians who participate in an MIPS APM are still evaluated on the four MIPS domains (quality, improvement activities, cost, and promoting interoperability), but the MIPS APM performance category weighting differs from the general MIPS scoring methodology, assigning “cost” a category weight of zero and providing higher weights for quality, improvement activities, and promoting interoperability. Unlike the general MIPS program, these weights do not change from year to year. MIPS APMs also allow participants to use quality measure reporting at the APM level, reducing the quality measure reporting burden for the individual physician or practice.
- Advanced APMs: These APMs also hold participants responsible for performance on cost and quality, but in addition require participants to assume downside financial risk. Advanced APM participants must also use 2015 Certified Electronic Health Record Technology (CEHRT). In exchange, Advanced Alternative Payment Models offer a 5% bonus, and allow clinicians to be excluded from MIPS reporting requirements. The APM itself will also offer APM-specific rewards based on its design. Clinicians can be eligible for advanced APMs if they meet certain threshold requirements for percentage of Medicare patients/percentage of Medicare Part B payments receiving care through the Advanced APM.
For more information, refer to the list of care models designated as MIPS APMs and Advanced APMs.
QPP Resources
The American Medical Association (AMA) offers podcasts, learning modules, and webinars to help physicians and their staff prepare for participation in the QPP.
Home Infusion Therapy Services
Medicare Learning Network article that provides guidance to providers and suppliers of home infusion therapy services about claims processing systems.
Medicare Utilization Data for Infectious Diseases Physicians
Please visit the Medicare Research, Statistics, Data & Systems Page for free and purchasable information, including utilization rates, cost reports, error rates, and beneficiary and provider surveys.